A 54-year-old suicidal patient presents to the ED after an unknown ingestion. Vitals are 98.9, 102, 18, 111/74, 97%, fs 98. She is somnolent but arousable. You send labs and find that the patient has an anion gap of 20, osmolal gap of 62, lactate of 8.8, ethanol of <10, and negative ketones.
Q: What are you concerned about?
A: The patient has a toxic alcohol ingestion of either methanol or ethylene glycol.
ˇThere are 4 main causes of osmolal gap: alcohols, sugars, lipids, and proteins. However, of concerning ingestants, only the toxic alcohols methanol and ethylene glycol will produce a concurrent anion gap acidosis.
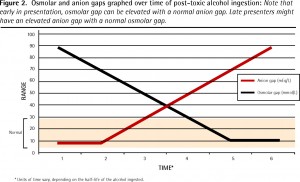
One thing to note is that the osmolal gap will fall as the anion gap rises. This is because the unmetabolized alcohol contributes to the osmolal gap, while the metabolites contribute to the anion gap. This makes the time of presentation important in considering the significance of these values. Additionally, the osmolal gap for a healthy person ranges from -12 to +12, so the physiologic gap may be different from the calculated gap.
Finally, the lactate could aid in differentiating between methanol and ethylene glycol ingestions. A very high lactate likely indicates that your hospital’s lactate analyzer is spuriously recording glycolate as lactate, thus implicating ethylene glycol. (They are structurally similar.) Although methanol’s metabolite, formate, induces the production of lactate, the spuriously elevated levels are usually much higher.
Either way, treatment for both methanol and ethylene glycol poisoning includes fomepizole, sodium bicarbonate, and hemodialysis. Cofactor supplementation is the only difference, with methanol ingestions requiring folic acid and ethylene glycol ingestions requiring pyridoxine and thiamine.
1) Wiener SW. Chapter 107. Toxic Alcohols. In: Nelson LS, etal. Goldfrank’s Toxicologic Emergencies. 9th ed. New York: McGraw-Hill; 2011
2) Shirey T, Sivilotti M. Reaction of lactate electrodes to glycolate. Crit Care Med 1999; 27:2305.
3) Hoffman RS et al. Osmol gaps revisited: Normal Values and Limitations. Clin Toxicol 1993; 31: 81-93.
4) Buckley NA, Whyte IM, Dawson AH. Utility of the osmolal gap. J Toxicol Clin Toxicol 1994; 32(1):93-95.
5) Patil N, Becker MWL, Ganetsky M. Toxic Alcohols: Not Always A Clear-Cut Diagnosis. Emergency Medicine Practice 2010; 12 (11).
6) LeBlanc C, Murphy M. Should I stay or should I go?: Toxic alcohol case in the emergency department. Canadian Family Physician 2009; 55(1): 46-49.
