SBO you say? 6-infinity hours until dispo?! Sometimes it feels like you want to just rub a lamp and all your dispo decisions would be granted!
Maybe it can!? Enter SBO and ultrasound!
What are you looking for on US? (Westafer & Faust 2015)

[Chao & Gharahbaghian]
[Chao & Gharahbaghian]
[Avila UOTW#20]
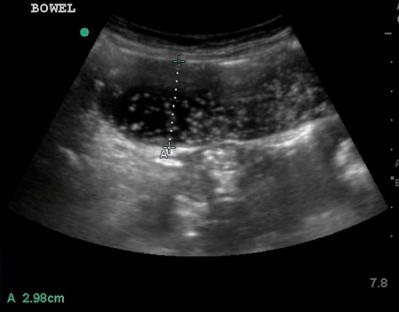
- Dilated loops of bowel > 2.5 cm in diameter in general but more specifically >2.5cm for jejunum and >1.5cm for ileum; while bowel distal to obstruction appears collapsed
- “To and fro” peristalsis on motion: decreased peristalsis
- The piano key sign: plicae circulares in the jejunum
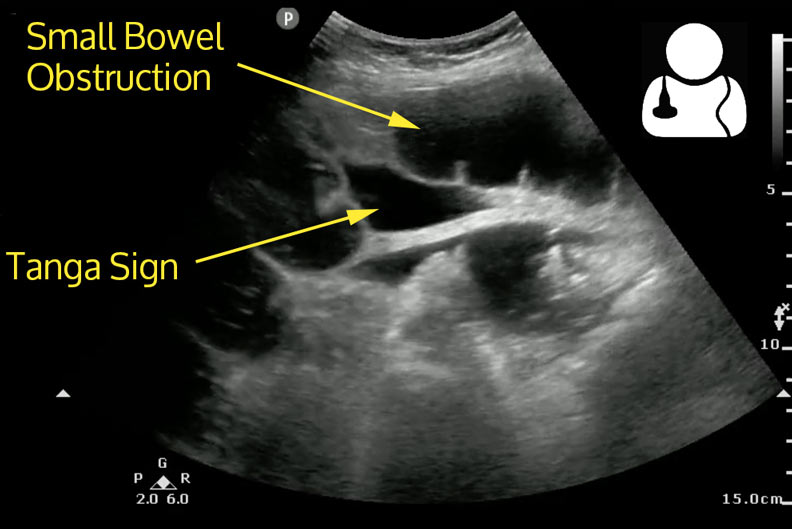
- Tanga sign: triangular shaped fluid collections between loops of bowel
- When to worry about small bowel ischemia? look for free fluid in bowel, no peristalsis, >3mm bowel wall thickening
How is it performed? http://5minsono.com/sbo/
- Select high frequency probe approx 3-5 MHz in large adults: Curvilinear, phased array, linear probe (skinny patients)
- “mowing a lawn” technique-move the probe up and down over abdomen (Probably better to watch video)
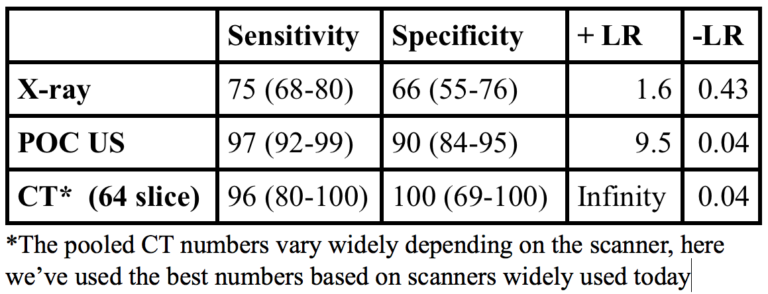
What does the literature say?
 [Foamcast SBO 2015]
[Foamcast SBO 2015]
Ulner et al 2010 looked at 174 patients in ER and found 52% had dx of SBO based on US and 48.3% had dx of SBO based on surgical pathology; 2.3% false positives on abd CT
Jang et al 2011 performed a prospective study in 76 ED patients w/ suspected SBO with plans for CT. Residents were given a 10 minute tutorial and 5 practice scans for SBO before performing it on the patients. A positive scan was found in 43% of patients. Sen&Spec for dilated bowel: 91%/84%; Sen&Spec for decreased peristalsis: 98%/27%
Taylor & Lalani 2013 performed a systematic review on the epidemiology of SBO in the ED and found that US although fewer studies was found to be superior to all other forms of imaging! [ +LR of 14.1 (95% CI = 3.57 to 55.66) and –LR of 0.13 (95% CI = 0.08 to 0.20) for formal scans and a +LR of 9.55 (95% CI = 2.16 to 42.21) and a –LR of 0.04 (95% CI = 0.01 to 0.13) for beside scans.]
RECAP:
- May provide rapid time to dispo for patient in ER
- Differentiating between ileus and obstruction difficult to discern on US
- Seeing dilated bowel may be more accurate for diagnosis than decreased peristalsis or intraperitoneal free fluid individually but having all 3 is even better!
Sources:
- Avila, J. http://www.ultrasoundoftheweek.com/uotw-20-answer/
- Alerhand, S. & Koyfman, A. Ultrasound for small bowel obstruction. 2014. http://www.emdocs.net/ultrasound-small-bowel-obstruction/
- Lin, M. Small bowel obstruction: Diagnosis by ultrasonography. 2014. https://www.aliem.com/2014/small-bowel-obstruction-diagnosis-ultrasonography/
- Westafer, L & Faust, J. 2015. Episode 23: SBO and Mesenteric Ischemia. http://foamcast.org/tag/small-bowel-obstruction/
- Unluer EE, Yavasi O, Erogul O, Yilmaz C, Akarca FK. Ultrasonography by emergency medicine and radiology residents for the diagnosis of small bowel obstruction. Eur J Emerg Med. 2010; 17:260–4.
- Avila, J. Small Bowel Obstruction. http://5minsono.com/sbo/
- Jang, T.B., D. Schindler, and A.H. Kaji, Bedside ultrasonography for the detection of small bowel obstruction in the emergency department. Emerg Med J, 2011. 28(8): p. 676-8.
- Taylor MR, Lalani N. Adult Small Bowel Obstruction. Acad Emerg Med. 2013;20:528-44.
- Chao, A. & Gharahbaghian, L. Tips and Tricks: Clinical Ultrasound for Small Bowel Obstruction – A Better Diagnostic Tool? https://www.acep.org/content.aspx?id=100218
- Kirschner, D. Sounding the Bowel. 2015. http://www.emresident.org/sounding-the-bowel/
*Shoutout to Taryn and Hayley for picking this up in a patient yesterday!
