Inspired by the procedural skills of Dr.’s Lazarciuc, Milliner, and Rajpal…
In brief, step by-by-step:
- Sterile field
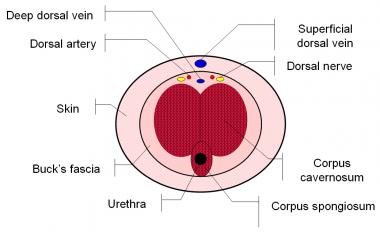
- Dorsal penile nerve block: 2 cc of Lidocaine w/o Epi injected close to penile base, from 2 and 10 o’clock aimed toward center of shaft.
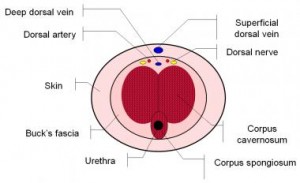
- Insert 19-gauge needle at 2 (and if needed, 10) o’clock. Can also use butterfly connected to syringe.
- Aspirate blood gas to confirm ischemic vs non-ischemic priapism (though this should be evident from H&P or darker-tinged venous blood).
- Aspirate using 20 cc syringe; repeat as needed. Can also leave needle in place and manually squeeze penis to extrude blood.
- If needed (i.e. blood clotting from prolonged symptom duration), place another needle proximally for normal saline syringe irrigation.
- As needed (and if without contraindications), put patient on monitor and inject 1 mL Phenylephrine 100 mcg/mL (pre-mixed here at Sinai) q3-5 min for 1 hr until symptom resolution. The alpha agonist activity contracts smooth muscle and permits venous outflow.
- Call Urology for shunt surgery if no detumescence by 1 hr. Specifically, a fistula is created between the corpus cavernosum and spongiosum, glans penis, or one of the penile veins.
- Do not forget to compress needle sites after their removal to avoid hematoma formation.