Left Bundle Branch Blocks (LBBBs) are scary because they can be confused for MIs and MIs are scary…almost as scary as Y2K. Which takes us back to the 90s…the good days, good music, great hairstyles, and Sgarbossa! 20 years ago we devised a rule to help distinguish a newly identified LBBB from MI, but in our post-Y2K world is there still room for improvement?

The Sens&Spec for the weighted (scored) Sgarbossa criteria is 50%/99% whereas the Sens&Spec for the unweighted Sgarbossa is 56%/94%. That’s the problem..the sensitivity of the Sgarbossa criteria is fairly low 50% with the unweighted being slightly better at 56%. The reasons for the low sensitivity may be 2/2 to a number of factors including: (1) reliance on a “point system”, (2) reliance on measurement cutoffs -5mm-for the discordant criteria instead of proportions, (3) AMI diagnosis made solely with biomarkers instead of angiographic evidence of occlusion.
Thankfully we have a post-Y2K solution to this: The Modified Sgarbossa Criteria! Introduced in 2012 by Dr. Stephen Smith.
His revised criteria eliminated the points system and focused on the following:
- Concordant ST-segment elevation ≥ 1 mm in any lead
- Concordant ST-segment depression ≥ 1 mm in lead V1 – V3
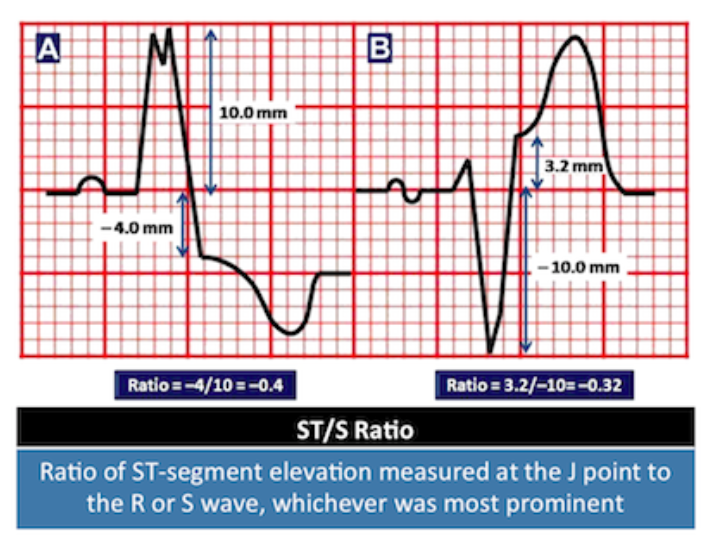
- Discordant ST/S Ratio ≤ -0.25
Presence of any one of these findings makes the patient fair game for cath. This study was validated by Meyers et al 2016 in a multicenter retrospective case-control review. They looked at patients with LBBB and one of the following: (1) acute coronary occlusion aka ACO (as documented on cath report), (2) elevated cardiac biomarkers with newly identified regional wall motion abnormality on echo, or (3) ECG positive for the modified Sgarbossa criteria with death before attempted cath. They had 45 patients w/ LBBB and evidence of ACO and 249 patients w/ LBBB and no evidence of ACO.
Their findings: Sens&Spec of 80%/99%! They even found lowering the cutoff to -0.20 improved sensitivity but decreased specificity however in the right clinical context using the lower cutoff may make more sense.
RECAP:
- The Modified Sgarbossa has a greater sensitivity 80% compared to 50-56% for the original Sgarbossa
- Using a lower discordant cutoff of -0.20 may be relevant in some patients with a high pretest probability for MI
- More studies!?
Sources:
- Rezaie, S. RebelEM. Modified Sgarbossa Criteria: Ready for Primetime? http://rebelem.com/modified-sgarbossa-criteria-ready-primetime/
- Meyers, H. P., Limkakeng, A. T., Jaffa, E. J., Patel, A., Theiling, B. J., Rezaie, S. R., … & Smith, S. W. (2015). Validation of the modified Sgarbossa criteria for acute coronary occlusion in the setting of left bundle branch block: A retrospective case-control study. American heart journal,170(6), 1255-1264.
