
Once you understand the basic functions of the components of your arterial line set-up and know how to position it properly the next level of mastery involves spotting other errors and optimizing them.
If you notice that your pulse pressure is very wide your patient may be severely volume depleted, they may have profound aortic insufficiency, or your arterial line may be lying to you. Alternatively, a very narrow pulse pressure can relay cardiac tamponade or an error in measurement. Here’s how, why, and how to fix it.
Why:
The fluid pressure wave the is transmitted to the arterial catheter and hydraulic tubing to displace the transducer and register as a blood pressure has a frequency which is expressed in cycles per unit time (beats per minute) and an amplitude of energy is expressed per beat until the wave reflects against the transducer. At certain lengths the wave is reflected back upon itself such the peaks and troughs of the waves (heartbeats) align exactly. This causes the amplitudes to be additive. The shortest distance that provokes this is described as the first harmonic and can be determined by the inverse of the wave’s frequency. As the wave travels along your tubing it expresses force against the wall of the tubing and expends energy. This causes the wave to “wind down” and is termed dampening. The analogy to describe this process is dropping a ball onto the ground: each time the ball bounces it expends more energy and each bounce is smaller until it comes to rest. How long it takes the ball to come to rest depends on the “hardness” of the ground, and this is termed the dampening constant. In your arterial line set-up this hardness constant is derived from the elasticity of the patient’s vasculature and of the IV tubing and stopcock system you use to conduct the pressure wave.
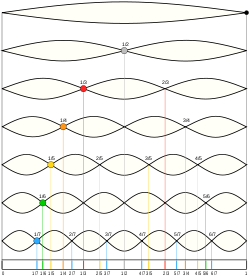
A figure demonstrating sign waves and harmonics.
How:
If the system is underdampened, harmonic waves develop and generate a blood pressure with a falsely extreme amplitudes (higher systolic and lower diastolic pressures than the patient is experiencing). Underdampending can be caused by excessively long and stiff IV tubing. You can detect underdampending on your waveform by looking for beats with a very rapid upstroke and a sharp, peaked appearance on your monitor. If the system is overdampened then excess friction leads the pressure wave to expend its energy early and promotes falsely narrow pulse pressures. Overdampending can be caused by bubbles within the tubing, kinks within the catheter, blood clots on or within the catheter, low volumes of fluid within the flush system, low pressure applied to the pressure bag. The good news is that the MAP (described by the midpoint in the sine wave of the heartbeat) is unchanged by these artifacts. However your systolic and diastolic blood pressures still yield clinical data and having gone through the trouble of placing an invasive monitoring system, you want them to be accurate.
The fix:
You can test to determine if your system is overdampened or underdampened by performing a square flush test. Do this by opening the continuous flus hvalve to create a square wave and observing the subsequent oscillations. If the system returns to baseline after one or two oscillations then the dampening of the system has been optimized. If there are more than one or two oscillations then the system is underdampened. If there are no oscillations then the system is overdampened.
Tubing should be exactly 4 feet to promote the correct length. Longer lengths of tubing can promote harmonics.
Use dedicate arterial pressure tubing when possible to maintain the appropriate compliance (“hardness”) of the walls of the system. Avoid large diameter tubing as this will lead to overdampening.
Remove air bubbles by flushing the line (flush to air rather than to the patient) or by aspirating them.
Tighten all connections.
Remove any excessive stopcocks.
Cheatham ML. Hemodynamic Monitoring: Principles to Practice. http://www.surgicalcriticalcare.net/Lectures/PDF/hemodynamic%20monitoring%20principles%20to%20practice.pdf. Updated 1/13/2009. Accessed 5/2/2016.
Nickson C. Life in the Fast Lane. http://lifeinthefastlane.com/ccc/arterial-line/. Updated 6/14/2015. Accessed 5/3/2016.
Yartsev A. Deranged physiology.comhttp://www.derangedphysiology.com/main/core-topics-intensive-care/haemodynamic-monitoring/Chapter%201.1.4/arterial-line-dynamic-response-testing. Updated 6/29/2015. Accessed 5/3/2016.
