Myxedema coma, or severe hypothyroidism, is an emergent condition with a high mortality rate (30-60%). Our patients rely on us to catch it early and treat aggressively. About 90% of cases occur during the winter months, and it is rarely seen in patients younger than 60.
Causes:
Myxedema coma is usually precipitated by another condition. Some of these include MI, infection/sepsis, stroke, PE, exposure to drugs that suppress the CNS, and prolonged exposure to cold. Note that 15% of patients who present with myxedema coma will have a temperature below 37 C, and of this group, 15% will have a temperature below 29.4 C.
What will we see?
Myxedema coma causes a physiologic perfect storm, because so many different systems are reliant on thyroid hormone. Decreased chronotropy and inotropy precipitate cardiogenic shock. Fluid retention exacerbates shock and causes hyponatremia. Hypothermia worsens chronotropy and inotropy further, and inhibits respiratory drive. Respiratory failure, cardiogenic shock, hyponatremia, and altered mental status produce the final clinical picture.
What does the ECG look like?
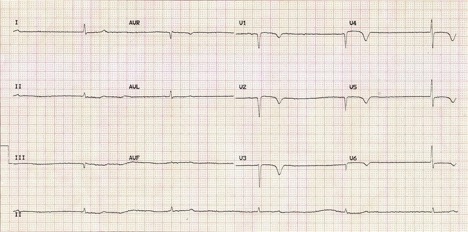
ECGs of myxedema coma patients have three classic features: 1) bradycardia, 2) low voltage, and 3) widespread T-wave inversions. Other possible features include QT prolongation, first degree AV block, or interventricular conduction delay.
How do we treat?
These patients require thyroid hormone (either T3 or T4). The decision on whether to give T3 or T4 depends on the patient’s age and comorbid conditions. Elderly patients and those with cardiac disease should get T4 (300-500 mcg bolus, or as a split bolus of 200-300 mcg 24 hours apart). Younger patients and those without any cardiac disease can get T3 (10-20 mcg bolus, then 10 mcg every hour for 24 hours). These patients also require steroids. Choose hydrocortisone for its dual mineralocorticoid and glucocorticoid effects (50-100 mg IV). Remember that in hypotensive patients, pressors often won’t work until after T3/T4 and steroids have been given.
References:
- Sharma AN, Levy DL. Thyroid and adrenal disorders. In: Marx JA, Hockberger RS, Walls RM, et al, eds. Rosen’s Emergency Medicine. 8th ed.
- Mathew V, Misgar RA, Ghosh S, et al. Myxedema coma: a new look into an old crisis. Journal of Thyroid Research. 2011.
- http://lifeinthefastlane.com/ecg-library/basics/hypothyroidism/
- Scott Weingart. Podcast 87 – Mind of the Resuscitationist: Stop Points. EMCrit Blog. Published on November 26, 2012. Accessed on February 20th 2017. Available at [https://emcrit.org/podcasts/stop-points/ ].
- Dubbs SB, Spangler R. Hypothyroidism: Causes, killers, and life-saving treatments. Emerg Med Clin N Am. 2014;32(2):303-17.
- Chu M, Seltzer TF. Myxedema coma induced by ingestion of raw bok choy. N Engl J Med. 2010;362(20):1945-6.
