The Interscalene Block
So, you want to provide local anesthesia to the patient with a broken clavicle or a dislocated shoulder. Maybe there’s a proximal / mid-humeral fracture or an injury over the deltoid. Whatever your needs may be, the interscalene block is an option for targeted anesthesia in the upper extremity to knock out parts of the brachial plexus. The short version of the procedure to accompany the pictures below is as follows: identify anatomy (specifically, the sternocleidomastoid muscle which will help landmark where the scalene muscles will be), identify interscalene area, and then infiltrate local anesthetic around the nerves. The video of the procedure at the end of the post is from ultrasoundpodcast.com.
The Patient’s Lateral Neck
(with SCM outlined)

The Angle of Needle Insertion
(lateral to SCM, but between anterior and middle scalene muscles)

Drawing of Anterior and Middle Scalene Muscles Next to SCM

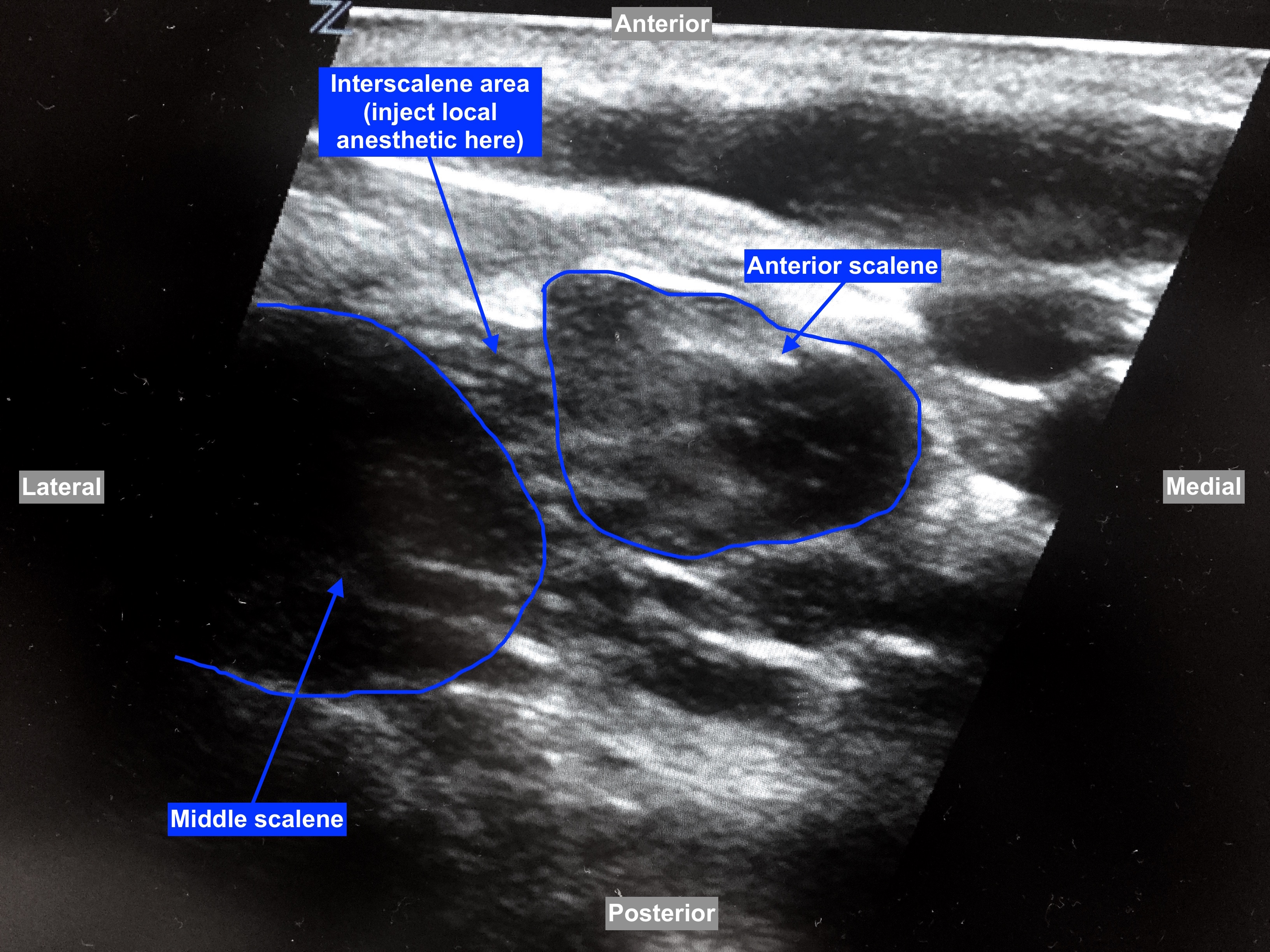
Interscalene Area on US
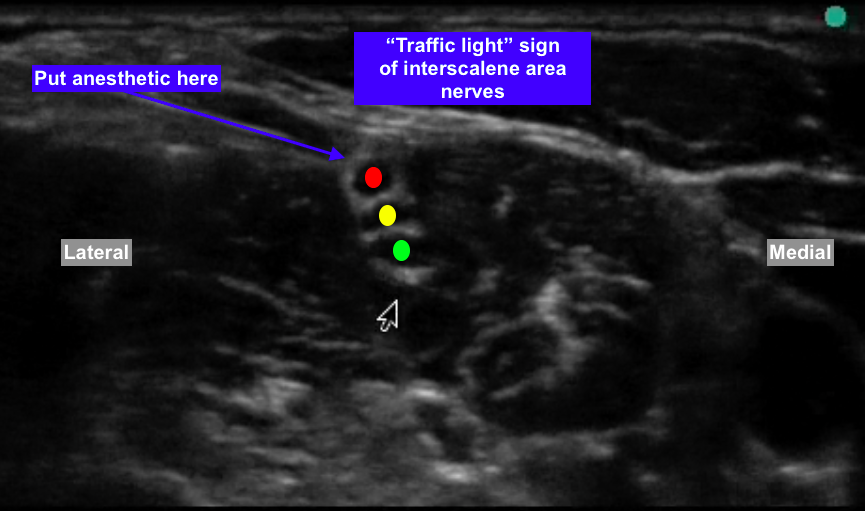
The Traffic Light Sign of Interscalene Area
The Procedure Video
(from the excellent UltrasoundPodcast.com)
The Procedure
Scan transversely in the area lateral to the sternocleidomastoid muscle (SCM) to identify the anterior and middle scalene muscles. The C5-C7 nerve roots are visualized as “traffic lights” vertically oriented between the two muscles. They are hypoechoic dark spots vertically stacked. Injecting about 10-15 mL of local anesthetic should provide anesthesia and analgesia. The (mild) motor and sensory deficits after the procedure affect the shoulder and upper arm.
Danger
Be sure to warn your patient about the following:
- temporary phrenic nerve paralysis
- recurrent laryngeal nerve blockade
- Horner’s syndrome

{kind=link}