Clinical Question – What’s a systematic approach you can use to improve your Echo?
Case – 66 M with IDDM, HTN, and obesity presents to Resus in septic shock. He is intubated for hypoxemic respiratory failure, and remains persistently hypotensive despite a fluid-challenge and 15 mcgs of levophed. You slap on the probe to evaluate his EF. Here’s the best image you can get:

This view (e.g. Mush) is not an uncommon view on a mechanically ventilated patient. You continue to flap the probe around but are unsuccessful in improving your echo. What should you do in order to improve your windows?
Strategies:
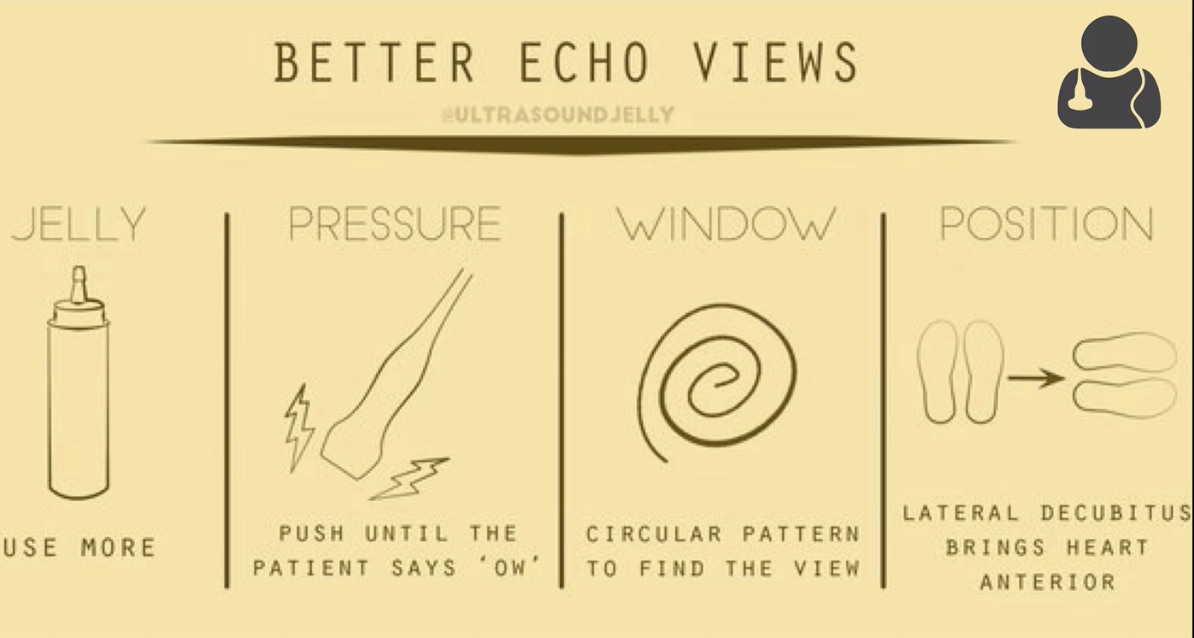
- General Strategies – use more gel, push the probe harder, and do a spiral pattern around the chest to locate the heart. Some patients can benefit from L lateral decube but this is impractical for the mechanically ventilated patient.
- Parasternal Long – Start as you normally do around the 3rd-4th ICS near the sternal border.
- Global View – Spiral around the chest to locate the heart.
- Fine-Tune the View – After you’ve found the heart, there are 3 fine motor movements you can do with the probe in order to get a crisper image.
- Twist – clockwise/counterclockwise
- Tilt – tilt the probe toward and away from you, and left to right
- Translate – move the probe up and down the chest to bring more of the heart onto the screen.
- Put it Together – Position probe at the 3rd/4th ICS at the sternal border. Do big sweeping spirals until you find what looks like the classic PSL. Twist/tilt/translate to perfect your view.
- Apical 4-Chamber – The best windows for the apical 4 chamber exist between the rib spaces. One way is to place the probe at the PMI for a normal Apical 4. If this fails, consider the alternative approach – start at the posterior axillary line at the 5th ICS and go midsternal to see if you can identify a 4-chamber view. If this fails, go up an additional rib space. This takes about 10-15 seconds. If you have no window, move on to the subcostal view.

- Subcostal – if you can’t get good parasternal windows, you may have an inferior shift of the heart. They may have excellent subcostal windows as a result.
- Technique – flatten the probe at the xiphoid process as much as possible to get the best view. You may need to tilt the probe toward the R shoulder to improve your view. Angle up or down to improve view. Ask the patient to take a big breath to bring the heart closer to the probe.
- Subcostal Short – substitutes for parasternal short. Turn probe 90 degrees counterclockwise (index toward patient’s head).
- Note – you shouldn’t make conclusions above ventricular/valve function based on one view. Confirm with an additional view.
Thanks Eric Chao and Neil Dubs for inspiring this post!
Resources – 5MinSono Optimizing Cardiac Views, Rob Arntfeld (Former SinaiEM US fellow!) – Echo Image Acquisition
