Clinical Scenario:
A 2-year-old female with no significant past medical history presents with vomiting and abdominal pain for 1 day. Among other entities in your differential diagnosis you are considering intussusception, however it is lower on your differential. How would you work-up this child?
Presenting Symptoms for Intussusception1
- Sudden onset of intermittent, severe, crampy, progressive abdominal pain
- Inconsolable crying and drawing up legs toward abdomen
- Vomiting, may become bilious
- Irritability
- Increasing lethargy
- Guaiac positive or grossly bloody stools, currant jelly stools
Plain Radiographs
Roskind et al studied 198 children 3 months to 36 months who underwent 3-view abdominal radiography for intussusception. The x-ray was compared with ultrasound, air enema, operative procedure, or improved clinical course. The study found 3-view abdominal x-ray was sensitive for ruling out intussusception.2 Limitations not withstanding, in patients with low clinical suspicion for intussusception plain radiographs may be considered.
- 3-view abdominal x-ray2
- Views: Supine, prone, left lateral decubitus
- Criteria to rule out intussusception:
- Air visualized in ascending colon in each view and transverse colon on supine
- Sensitivity 100% (95% CI, 79.1-100)
- Specificity 17.4%
- Negative predictive value 100% (95% CI, 79.1-100)
- 2-view abdominal x-ray with air in the ascending colon
- Sensitivity 89.5% (95% CI, 75.7-100%)
- Specificity
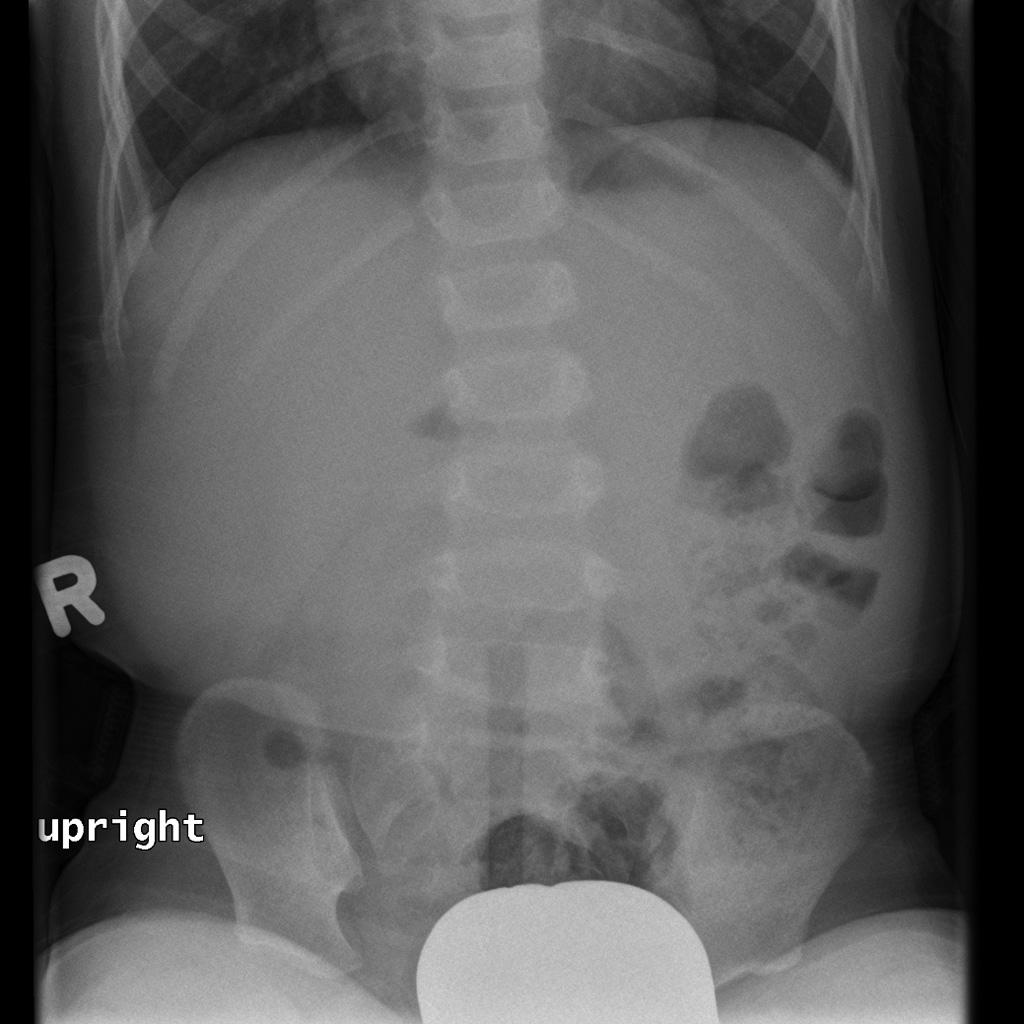
Case courtesy of Dr Angela Byrne, Radiopaedia.org, rID: 8113
Ultrasound
Ultrasound is often a definitive study for intussusception given it has a high sensitivity/specificity, is non-invasive, and does utilize ionizing radiation. Although classically performed by radiology, the use by emergency physicians is increasing.3-7
- Linear, high-frequency (5-10 MHz) transducer
- Child is placed supine in a position of comfort
- Technique 1
- Follow the ascending to transverse colon
- Transducer placed in the right lower quadrant with indicator oriented toward the patient’s right side
- Sweep the probe superiorly along the right side of the abdomen
- Upon reaching the right upper quadrant the indicator should be oriented toward the patient’s head.
- *Make sure to search carefully in the RUQ since this is where the majority of intussusceptions may be found (80%)
- Sweep the probe laterally toward the epigastrium
- Technique 2 – “Lawnmower”
- Scan the entire abdomen in a systemic manner, up and down like a lawnmower
- Once the intussusception is found it should be imaged in the transverse and longitudinal views
- Findings
- Soft tissue mass in right mid abdomen
- Transverse cut: “target” or “donut” sign
- Longitudinal cut: “cresecent”sign or “pseudokidney” sign
https://youtu.be/o0kyD9ZmD4I
- Radiology8
- Sensitivity: 98-100%
- Specificity: 88-100%
- POCUS7
- Sensitivity: 85 % (95 % CI 54, 97 %)
- Specificity: 97 % (95% CI 89, 99 %)
Take Away Points:
- In children with a low suspicion for intussusception 3-view abdominal x-rays may help rule out the diagnosis
- Ultrasound for intussusception is sensitive and specific
References
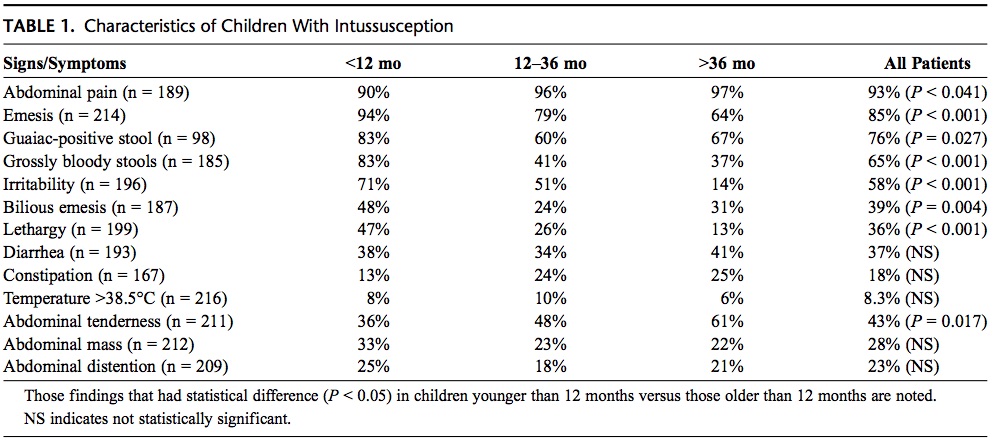
- Mandeville K, Chien M, Willyerd FA, Mandell G, Hostetler MA, Bulloch B. Intussusception: clinical presentations and imaging characteristics. Pediatr Emerg Care. 2012;28(9):842-844.
- Roskind CG, Kamdar G, Ruzal-Shapiro CB, Bennett JE, Dayan PS. Accuracy of plain radiographs to exclude the diagnosis of intussusception. Pediatr Emerg Care. 2012;28(9):855-858.
- POCUS4PEDS. https://www.youtube.com/channel/UC4t0bJTDBJeFiEPMkHN-ZtA.
- Doniger SJ, Salmon M, Lewiss RE. Point-of-Care Ultrasonography for the Rapid Diagnosis of Intussusception: A Case Series. Pediatr Emerg Care. 2016;32(5):340-342.
- Halm BM, Boychuk RB, Franke AA. Diagnosis of intussusception using point-of-care ultrasound in the pediatric ED: a case report. Am J Emerg Med. 2011;29(3):354 e351-353.
- Marin JR, Abo AM, Arroyo AC, et al. Pediatric emergency medicine point-of-care ultrasound: summary of the evidence. Crit Ultrasound J. 2016;8(1):16.
- Riera A, Hsiao AL, Langhan ML, Goodman TR, Chen L. Diagnosis of intussusception by physician novice sonographers in the emergency department. Ann Emerg Med. 2012;60(3):264-268.
- Applegate KE. Intussusception in children: evidence-based diagnosis and treatment. Pediatr Radiol. 2009;39 Suppl 2:S140-143.
