In case you haven’t gotten to this month’s EM:RAP, there’s a really great segment on an important ED procedure that we definitely don’t do enough of in the ED: the nerve block. The section discusses the femoral nerve block and how to perform a fascia iliaca compartment block (the “3-in-1” block)–which hits 3 major nerves that supply the leg: the femoral nerve, the obturator nerve, and the lateral femoral cutaneous nerve.
This block is fantastic for controlling pain from isolated hip/femur fractures. We see these fairly frequently in elderly patients, and using a nerve block will not only allow for excellent pain control, but it also prevents over-utilizing opioid medications, which may be especially dangerous in the geriatric population.
Here’s how to do it:
-
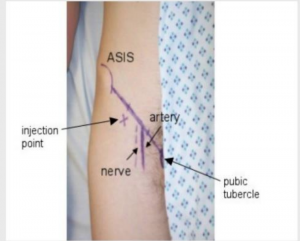
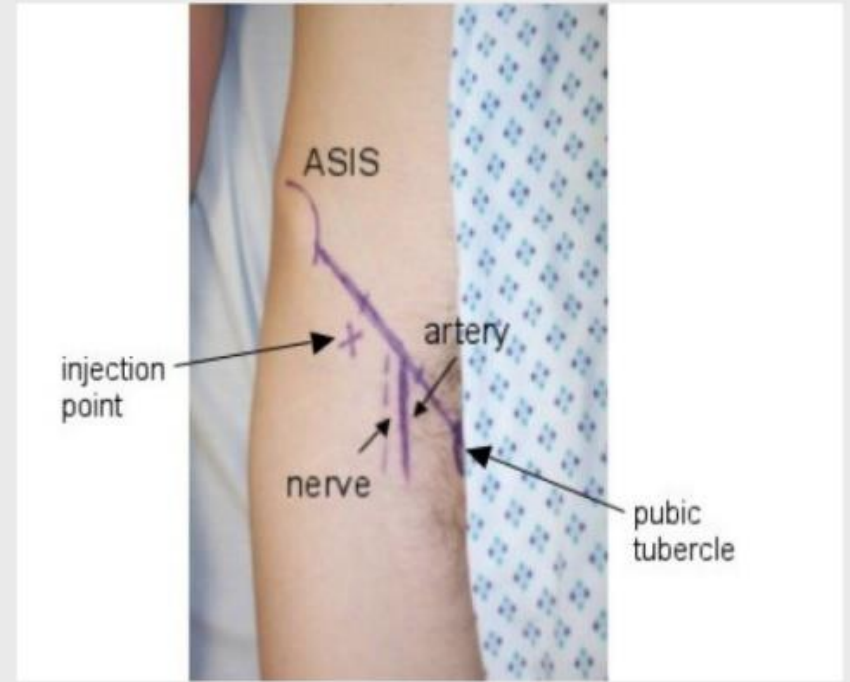
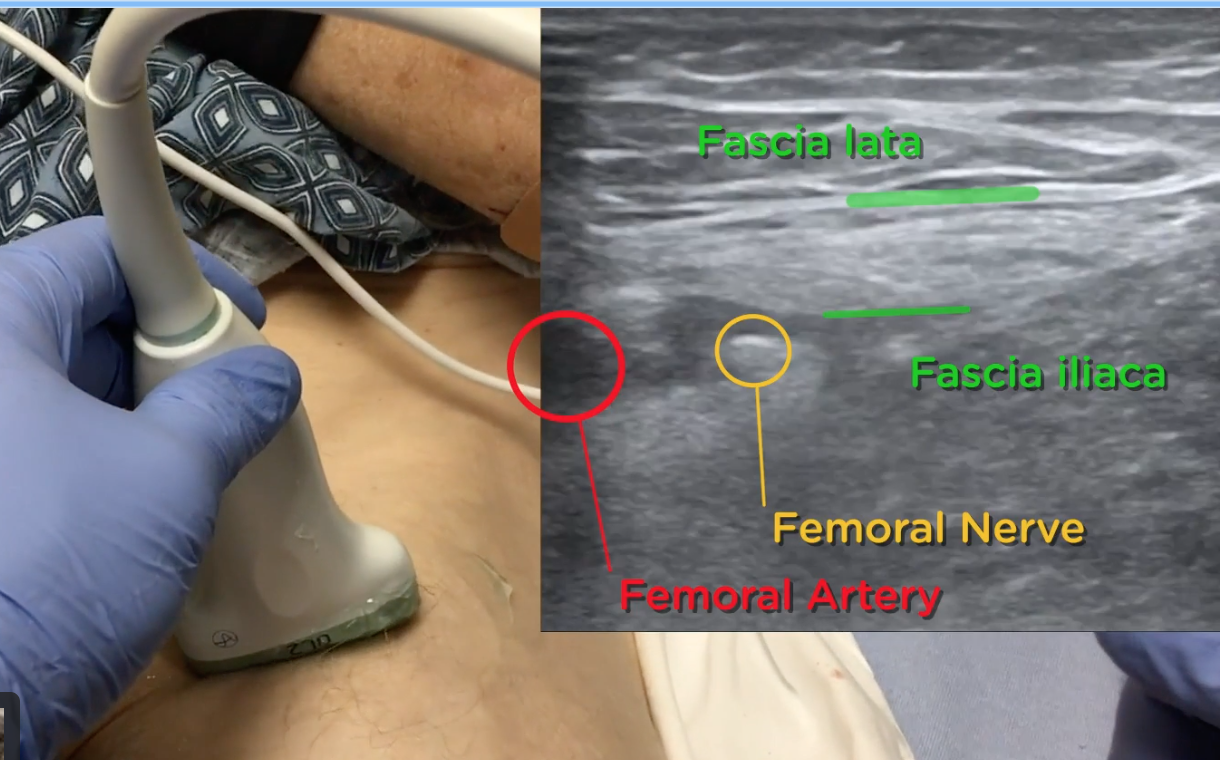
- Identify your landmarks: draw an imaginary line from the ASIS to the pubic symphysis. Identify your femoral artery, by either feeling for the pulse or using your ultrasound probe. Your femoral nerve will be immediately lateral to this.
- Prep the patient: chlorhexidine the skin, put a probe cover on your transducer.
- Choose your meds: bupivacaine is longer acting than lidocaine, so you likely won’t need to redose. You’re going to want about 20-30cc total. Create a wheal just under the skin at the injection point.
- Landmark approach:
- Divide your line from the ASIS to the pubic symphysis into 3rds. Your injection point will be at the junction of the lateral ⅓rd and medial 1/3rd
- Inject SUPERIORLY (lowers your risk of hitting the artery), aspirating as you go
- Ultrasound-guided:
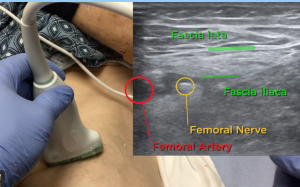
- Look for the bright white, honeycomb appearing structure lateral to the artery.
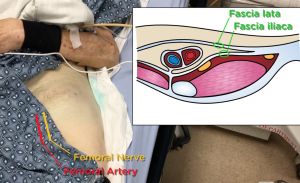
- Insert your needle parallel to the inguinal ligament and visualize it passing through both fascial layers. Watch as you inject the anesthesia, look for muscle separating from the fascia.
- Identify your landmarks: draw an imaginary line from the ASIS to the pubic symphysis. Identify your femoral artery, by either feeling for the pulse or using your ultrasound probe. Your femoral nerve will be immediately lateral to this.

By injecting into this compartment, the goal is that the medication will track up the fascial planes and into the fascial compartment, bathing the obturator nerve and lateral femoral cutaneous nerves as well as the femoral nerve–providing outstanding pain control.
A few things to remember:
- Don’t use this in a patient with multi-trauma to the pelvis/lower extremities or if there’s any concern for compartment syndrome.
- Avoid this procedure in patients on anticoagulation or with elevated INRs
- Max safe dose: 2mg/kg of bupivacaine, 4mg/kg of lidocaine
Sources:
–https://www.emrap.org/episode/fasciailiaca/fasciailiaca <<<<EXCELLENT VIDEO HERE!!
