The intraosseous line. What a beautiful solution to so many problems. Let’s take a minute to reflect on the IO, what it can do, how to do it, and to assuage your fears of complications.
When to use an IO: If you think, “should we put in an IO?” Then, YES, yes you should!
The rule of thumb is, if you think about using an IO, its time to use an IO! If you have a sick patient with difficult IV access and have any urgent need for intervention, then yes, an IO is a great answer. It is not only for patients in cardiac arrest. Think about it when you have an ESRD patient coming in with hyperkalemia, a seizing patient, a severely dehydrated patient with sepsis, a crashing patient needing pressors now, or a critical peds patient. It is faster than an IV and works as a central line. If you think about it, use it!
What can I give through an IO: Literally anything! Fluids, pressors, any medication. It is your 10 second central line.
But what if I need labs? Most labs can be drawn from an IO. The WBCs, platelets, potassium, calcium and LFTs may be off. But, everything else should be accurate.
When can I not use an IO: The answer is basically never. But, sometimes you need to choose a different IO site. Don’t put an IO in a fractured bone, on a limb with a vascular injury, or a place where there is overlying cellulitis, burns or osteomyelitis. If you fail once, use a different site. You cannot try a second IO in the same site. Also, relatively contraindicated in kids with osteogenesis imperfect and with right-to-left intracardiac shunts (because those kids are at higher risk for cerebral fat or bone marrow emboli).
Complications: the complication rate of IOs is small and similar to IV access! Small risk of infection / osteomyelitis. Small risk of compartment syndrome if large volumes infused into IO that is incorrectly placed into the subcutaneous tissue.
How do I put in an IO?
- douse the area in betadine or chlohexadine
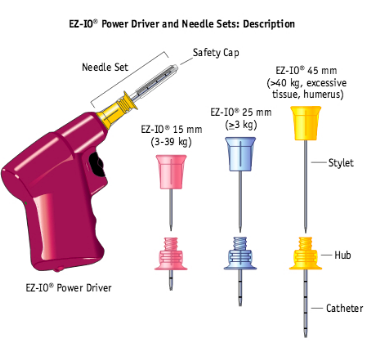
- drill in needle
- pink for peds
- blue for normal
- yellow for fat
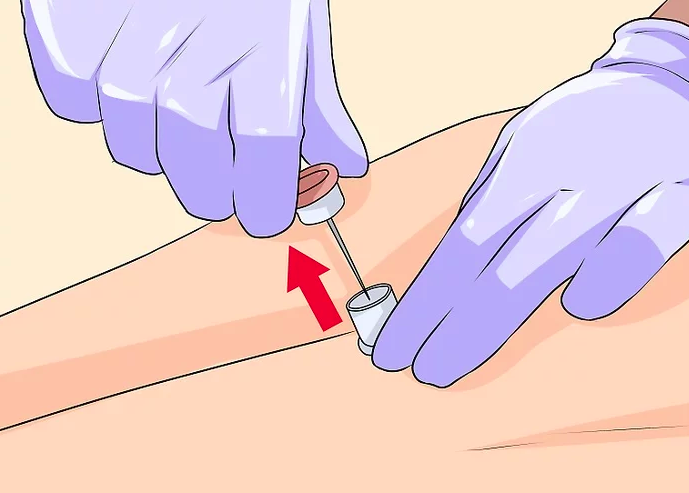
- unscrew the trochar
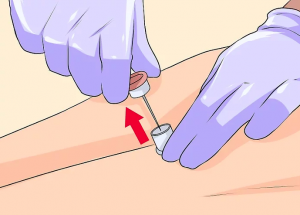
- screw in catheter hub
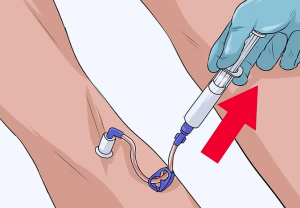
- aspirate
- flush
- You’re done!

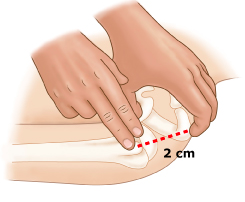
Sites:
- Proximal Tibia: 2 cm below tibial tuberosity
- Proximal Humerus: greater tubercle of the proximal humerus, 2 cm below acromion process
- Manubrium: superior 1/3 of sternum
- Distal femur: 1-2 cm above patella
- Medial malleolus: 1-2cm superior to the medial mal
Watch a video to learn how to place an IO:
https://www.youtube.com/watch?v=KHXSfh2ZRDM
Want to read more?
https://www.uptodate.com/contents/intraosseous-infusion
https://lifeinthefastlane.com/ccc/intraosseous-needle-insertion/
