In 2016, ACEP published “Clinical Policy: Critical Issues in the Evaluation of Adult Patients with Suspected Transient Ischemic Attack (TIA) in the Emergency Department” in the Annals of EM. Here is a brief refresher.
Transient ischemic attack (TIA) is a part of a spectrum of ischemia affecting the central nervous system.
- “Transient episode of neurologic dysfunction caused by focal brain, spinal cord, or retinal ischemia, without acute infarction.” – The American Heart and Stroke Associations
- Most TIAs are thought to last fewer than 1-2 hours.
- Currently there is no specific acute intervention for patients with TIA; the goal is to reduce the potential for future strokes.
TL;DR Summary (more detail below)
In addition to working in collaboration with your neurology colleagues, the next time you treat a patient suspected of having a TIA, follow these ACEP clinical recommendations:
- Do not discharge the patient.
- Do not delay neuroimaging.
- Consider ED observation for patients without high-risk conditions* to evaluate those at short-term risk for stroke.
Are there clinical decision rules that can identify patients at very low short-term risk for stroke who can be safely discharge from the ED?
- Do not rely on existing risk stratification instruments (ex – ABCD2 score) to identify TIA patients who can be safely discharged.
- ABCD2 score – https://www.stroke.org/sites/default/files/resources/tia-abcd2-tool.pdf
- Level B recommendation
In adult patients with a suspected TIA, what imaging can be safely delayed from the initial ED workup?
- The safety of delaying neuroimaging from the initial ED workup is unknown. If noncon brain MRI is not readily available, it is reasonable for physicians to obtain a noncontrast head CT as part of the initial TIA workup to identify TIA mimics (ICH, mass lesion). However, NCHCT should not be used to identify patients at high short-term risk for stroke.
- Level C recommendation
Is carotid ultrasonography as accurate as neck CTA or MRA?
- Carotid US may be used to exclude severe carotid stenosis because it has accuracy similar to that of MRA or CTA.
- Level C recommendation
Can a rapid ED-based diagnostic protocol (ex, ED observation unit) safely identify patients at short term risk for stroke?
- In adult patients with suspected TIA without high-risk conditions*, a rapid ED-based diagnostic protocol may be used to evaluate patients at short-term risk for stroke.
- High risk conditions: abnormal initial CT, suspected embolic source, carotid stenosis, previous large CVA, or crescendo TIA
- Level B recommendation
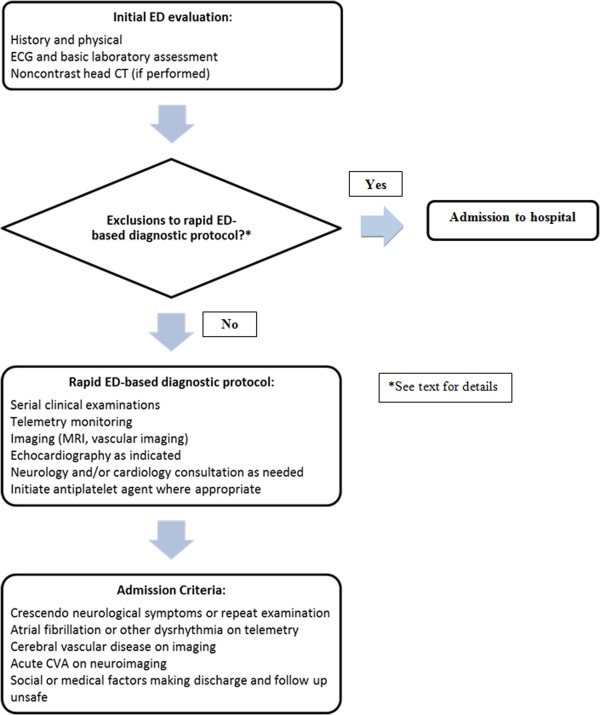
An example of a rapid ED-based diagnostic protocol
You can download and read the entire clinical policy here: https://www.acep.org/Physician-Resources/Policies/Clinical-policies/Clinical-Policy-Suspected-Transient-Ischemic-Attack/
