Acute non-traumatic temporomandibular joint (TMJ) dislocations occur after extreme opening of the mouth (yawning, eating, laughing, singing or dental treatment. TMJ dislocation is when the anterior condyle moves too anteriorly and becomes locked in the eminence. This also results in stretching of ligaments and is associated with severe spasm that results in difficulty closing the mouth that further inhibits the condyle from moving back into the mandibular fossa.
Diagnosis is clinical, if traumatic or concern for fracture imaging should be obtained. Patients will need reduction. This can be done by ED physicians, but a certain subset should be referred to oral surgeons: dislocation with associated fracture, superior or posterior dislocation, failed reduction despite multiple attempts.
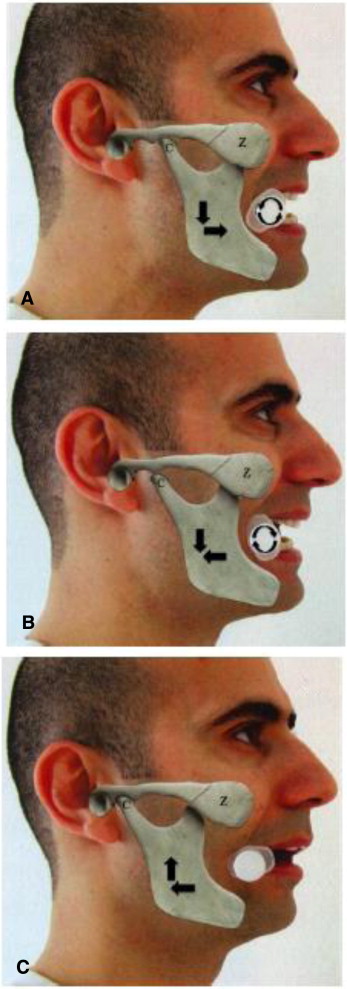
There are a number of different manual reduction techniques, including the classic intra-oral reduction approach, in which the practitioner applies downward force and then guides mandible posteriorly and superiorly back into place (as seen below), however this may require procedural sedation.

The syringe technique can quickly reduce a TMJ dislocation without the use of sedation. This technique requires a 5 or 10ml syringe that is placed between the posterior upper or lower molars on one of the affected sides. The patient should gently bite down and roll the syringe back and forth between the teeth until reduction is achieved. The opposite side reduces spontaneously, however, if this does not occur, the syringe should be placed on that side as well. Small case series have shown success with this technique.
Sources:
Gorchynski J, Karabidian E, Sanchez M. The “syringe” technique: a hands-free approach for the reduction of acute nontraumatic temporomandibular dislocations in the emergency department. J Emerg Med. 2014 Dec;47(6):676-81.
