Intro
You are working a BNT shift at Elmhurst and you pick up a patient who is complaining of neck pain after a fall. Do they need to be in a c-collar? Should you order a CT c-spine? What are the unstable c-spine injuries you are looking for?
Shout out to Rozy for trying to teach me this when I was an intern, and Angela, who recently attempted to pimp me on this topic and inspired this TR pearl.
tl;dr (<5 minutes)
There are two clinical criteria used to determine the need for radiographic imaging – Canadian and Nexus C-spine. It is important to remember that the Nexus criteria does not include mechanism or age of the patient.
The ABC’S of reading a CT C-spine: Alignment, Bones, Cartilage, and Soft tissue. If you only have 15 seconds before the next trauma comes in: pull up the sagittal view, scroll to the midline and run down each of the four smooth lordotic curved lines (see image in extended pearls). You will catch 90% of unstable fractures in the first sweep, then you can come back and do a more thorough review when the dust settles. Read your own scans…
Unstable C-spine injuries: “Jefferson Bit Off A Hangman’s Thumb”
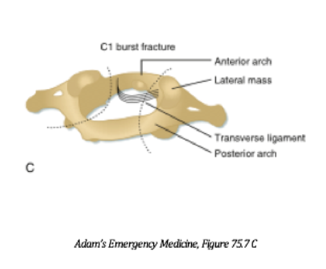
- Jefferson Burst Fracture
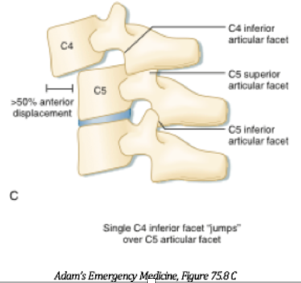
- Bilateral Facet Dislocation
- Odontoid Type II and III Fracture
- Atlanto-occipital Dislocation
- Hangman’s Fracture
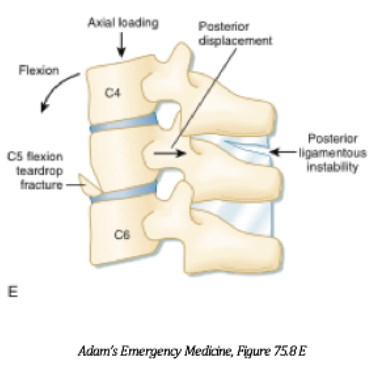
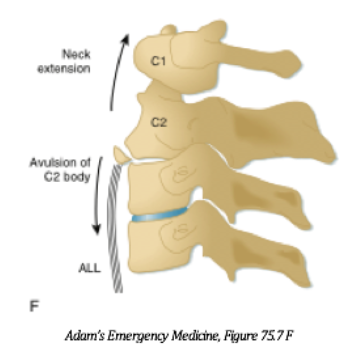
- Teardrop Fracture
Extended Pearls – (>5 minutes)
Canadian C-spine: Utilizes three categories to determine if the cervical spine can be clinically cleared without imaging.
- Age greater than or equal to 65, extremity paresthesias, or dangerous mechanism.
If Yes → this is a high risk patient and imaging is recommended. If No →
- Low risk factor present – requires at least one to be present. So it’s an OR, not an AND: Sitting position in the ED, ambulatory at any time, delayed (not immediate onset) neck pain, no midline tenderness, simple rear end MVC.
If Yes → proceed to the next criteria. If No → imaging is recommended.
- Able to actively rotate the neck 45 degrees left and right.
If Yes → patient is low risk and no imaging required. If No → obtain CT c-spine
“Canadian CT C-spine is a powerful, sensitive tool but remember that it cannot be used for all patients. The original study only included patients who were alert, with GCS 15 and stable with SBP>90, RR10-24. However, when used appropriately, the CT c-spine rule has been shown to be almost 100% sensitive and 42.5% specific for identifying clinically important C-spine injuries.”
Nexus C-spine: Utilizes five criteria, if any of the criteria are present the c-spine cannot be cleared and imaging should be considered.
- Focal neurological deficit
- Midline spinal tenderness present
- Altered level of consciousness present
- Intoxication present
- Distracting injury present
What qualifies as a distracting injury? Distracting injury includes a long bone fracture, a large burn, a crush injury, or any other injury you anticipate will require surgical management. There is debate on whether a distracting injury actually increases the risk of missing a c-spine injury.
It is also important to remember that the Nexus criteria does not include mechanism or age of the patient. However, if you use the Canadian CT c-spine rule for patients over the age of 65, they are automatically considered high risk.
k, so you decide to get a CT scan and the imaging is done. Unfortunately, VRADs is backed up and you are unable to get an official read…or the patient is adamantly attempting to remove their c-collar prior to the read…or it is read as negative but the patient is still complaining of severe pain…
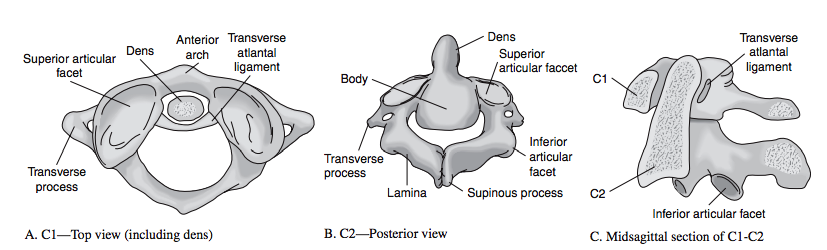
Quick review on cervical spine anatomy: There is anatomical variation between the seven cervical vertebrae, particularly C1 and C2.
- C1 – “Atlas”: Articulates with the occiput allowing for head flexion and extension. C1 does not have a body or spinous process, instead holds the dens of C2.
- C2 – “Axis”: Articulates with C1 to allow for lateral head movement. Dens articulates with the anterior arch of C1 via the transverse atlantal ligament.
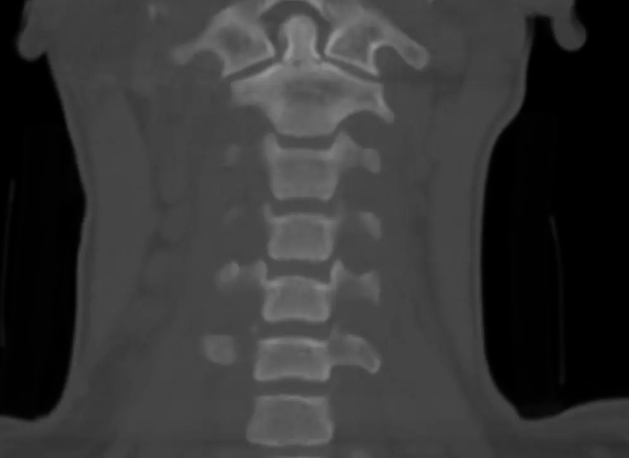
The ABC’s of reading a CT c-spine – You need to look at all three CT views for a systematic approach to reading a CT c-spine including sagittal, coronal, and axial views.
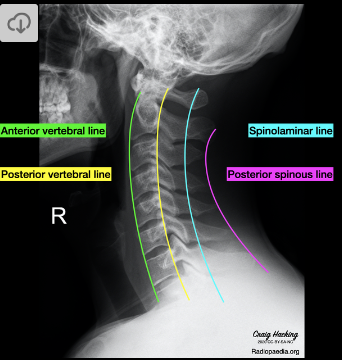
Alignment: View the alignment of the 4 smooth lines best visualized in the sagittal view -similar to a lateral view on x-ray.
- Anterior portion of vertebral body
- Posterior vertebral body
- Spinolaminar lines
- Tips of spinous processes
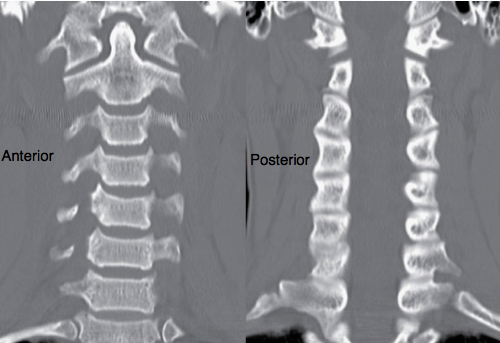
Bones: Should be visualized in all three views for any fractures or chipped pieces of bone.

Cartilage: Evaluate for widening, narrowing or asymmetry between vertebral bodies and spinous processes (most useful are sagittal and axial views).
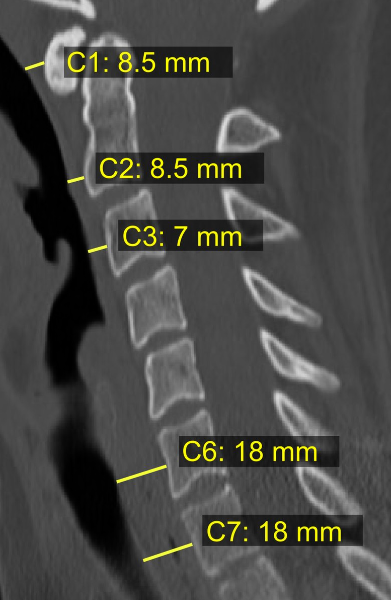
Soft tissue: Grossly evaluate prevertebral soft tissue (retropharyngeal space) in the sagittal view (narrow approx 5-10mm from C1-C4, thickens around C5 where the esophagus lies anteriorly). Soft tissue swelling may hint towards a fracture but its absence does not exclude injury.
Unstable C-spine injuries: “Jefferson Bit Off A Hangman’s Thumb”
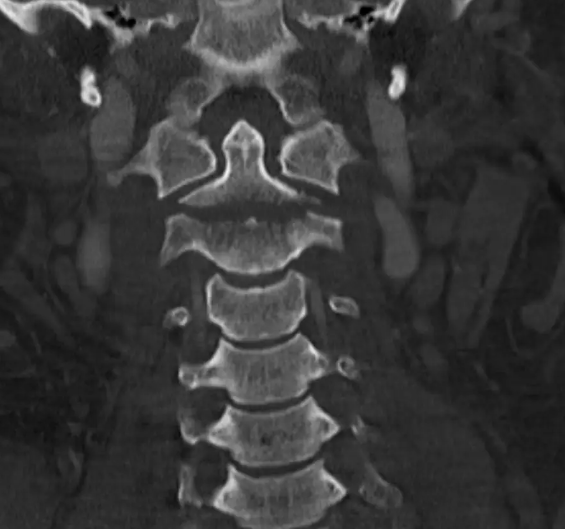
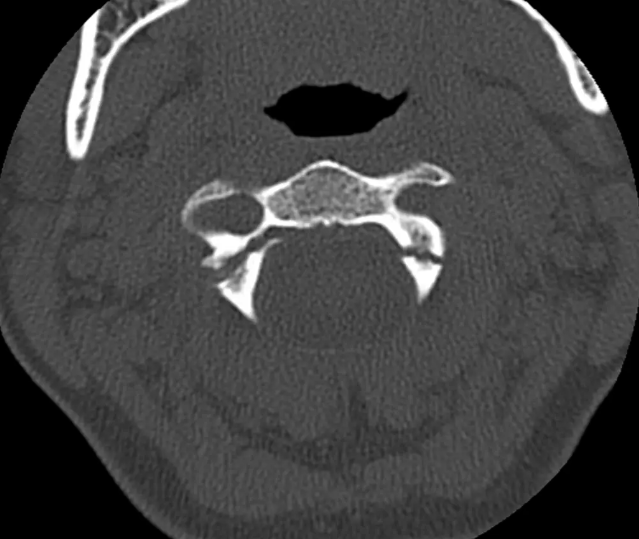
1. Jefferson Burst Fracture (C1): Burst fracture of anterior or posterior arch of C1. Caused by axial vertical compression. Fractured bony fragments can compress the spinal cord and be fatal. Can also disrupt the transverse ligament.

2. Bilateral Facet Dislocation: Anterior displacement of the superior vertebral body (>50%) over the inferior vertebral body. Caused by hyperflexion injury that can be caused by rapid deceleration. Can disrupt the anterior/posterior ligaments and compress spinal cord due to significant displacement.
3. Odontoid (dens) Type II and Type III Fracture (C2):
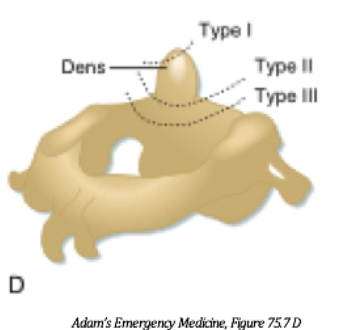
Type II: Fracture of C2 at the base of the dens, does not affect the vertebral body.

Type III: Fracture of C2 dens with extension into the C2 vertebral body.

4. Atlanto-occipital Dislocation: Flexion injury that causes destabilization of transverse ligament holding atlas and occiput together. Usually fatal.
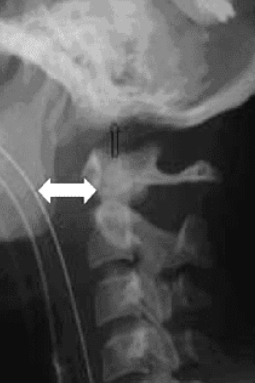
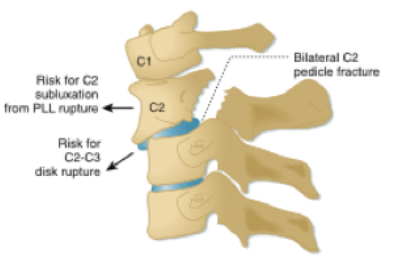
5. Hangman’s Fracture (C2): C2 pedicle fracture caused by extension injury with anterior slippage of C2 vertebral body.

6. Teardrop Fracture: Hyperextension or flexion injury causing avulsion of vertebral body, can occur at any cervical level.

Further Resources
Rosen’s Chapter 36: Spinal Injuries
Emergency Radiology: Case studies – Part 5 Cervical Spine Radiology
https://www.ncbi.nlm.nih.gov/books/NBK539734/ https://www.nejm.org/doi/full/10.1056/nejmoa031375
