Super cool case, admittedly, maybe not a super high yield diagnosis BUT, I hope we can all agree, still very dope.
Case: CC: 46yo M p/w worsening b/l vision over 1mo, now blind.
Vitals: WNL
PMHx: L eye global rupture ~6mos ago 2/2 nail penetration requiring repair
Pertinent HPI: First noticed previously injured L eye VA worsening, then good R eye becoming progressively blurrier until now completely blind. No recent trauma or other symptoms including eye pain/itchiness, headaches, fevers, chills, or other neuro complaints. No substance/etoh use.
Pertinent ED Exam Findings: No pupillary response in R eye, complete blindness, otherwise unremarkable. Conjunctival injections and corneal hazing to L eye, only able to appreciate dim lights and vague blurry shapes.
Ophtho Exam: Papilledema and nonreactive pupil in R eye. Possible blurred disc margins, conjunctival injections, and post-op sutures in L eye.
Work-Up: Labs unremarkable, aside for +RPR (pt endorsed a prior hx of treated syphilis). CTH+ shown below read as “irregular contrast-enhancing cystic lesions scattered throughout brain including subarachnoid space with moderate hydrocephalus and chronic infarct of R posterior parietal lobe”. Eventual MRI showing optic chasm displacement due to cystic lesions in the suprasellar region.
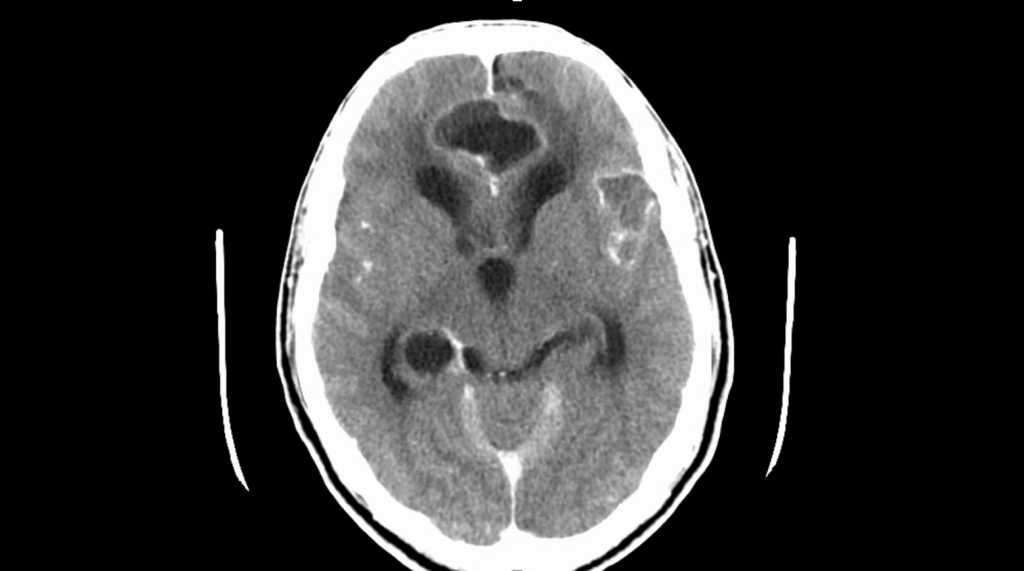
Diagnosis: Neurocysticercosis!
– Caused by larval stage of pork tapeworm, Taenia solium
– Endemic to many regions of Central & South America, sub-Saharan Africa, India, and Asia, particularly in pig-raising communities
– “Neglected tropical disease”: largely affecting impoverished, rural communites
– Thought to affect ~50 million people worldwide
– Considered to be one of the most common etiologies for new-onset seizures in young adults in aforementioned communities
– Usually ingestion of eggs in undercooked pork, grows in small intestines, more eggs shed and transmitted in human feces
– Initial phase largely asx, can be that way for several years
– Thought to inhibit cellular immune defenses and cannot be killed via humoral antibodies
– Eventually loses this evasive ability, which is when the body attacks these cystic colonies, causing the classic contrast-enhancing lesions
Symptoms: dependent on location of lesions
– Intraparenchymal: >60% cases, nonspecific neuro findings based on location of lesions (i.e. seizures, visual changes, n/v, weakness/numbness, meningitis/encephalitis)
– Extraparenchymal: again varies on location, depending on if lesions are in subarachnoid, spinal, ocular, or ventricular space
Work-Up: Labs usually nonspecific, imaging via CTH+ and/or MRI, serology
Management:
– Dexamethasone: 0.2-0.4mg/kg for inflammation
– Antiparasite: Albendazole 15mg/kg divided in 2 doses up to 1200mg per day (for 1-2 lesions) + praziquantel 50mg/kg per day divided in 3 doses (if 3+ lesions) for 10-14d*
– Antiseizure ppx
– Hydrocephalus management (i.e. VP shunt) if necessary
* Antiparasitic medication is contraindicated if signs of cysticercal encephalitis given may worsen inflammation and cause worsening cerebral edema and possible herniation
Hope you enjoyed the case! Be sure to cook your pork and consider cysticercosis in your ddx for new neurological sx, particularly in our Elmhurst population.
