Of the three primary locations for central line placements, most EM residents seem to be least well-versed in the now rarely placed subclavian central line. The feared complication of pneumothorax steers many doctors to other locales. But there is a time and a place for everything, so knowing how to improve your chance of successfully placing a subclavian line without complication will serve you well with your next neckless and morbidly obese patient requiring central access.
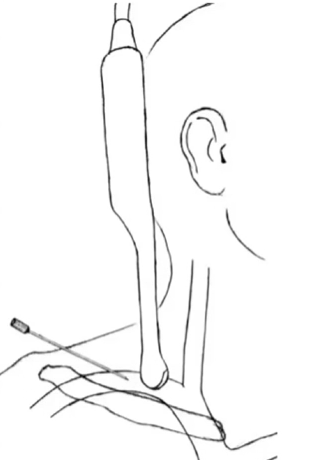
Not surprisingly, dynamic ultrasound guidance decreases the failed catherization rate (17.9% to 2.9%) and the complication rate (29.9% to 10.6%)* for subclavian central line placement when compared to landmark guidance. This is backed up by a meta-analysis written by our very own Jeremy Kim. The three main modes of ultrasound visualization are shown below: infraclavicular, supraclavicular, and “pocket shot”, followed by an excellent video overview of the basic approach to ultrasound guided subclavian line placement. Once visualized, the approach is essentially the same as other soon guided central line approaches, perhaps with a greater emphasis on the longitudinal view to avoid back-walling the needle/guidewire into the lung.
Supraclavicular

Infraclavicular

Pocket shot
*this is for all complications, not just pneumothorax
http://www.annemergmed.com/article/S0196-0644%2815%2900578-8/pdf#page=1&zoom=auto,-71,552
