You are in RESUS feeling like a boss (either it’s your last RESUS shift because you’re becoming a senior, you have finally made i through 2nd year and have learned how to tell Gueldye “no”, or are finally reaching the end of endless streaks of B-side nights as an intern). In rolls EMS with a super sick hypotensive patient coming from a nursing home with no information except that he is altered and hypotensive.
Is it septic shock? Or cardiogenic shock? Or something else? You intubate, place a central line, start pressors and put in a foley. He is stable-ish when you step back and try to think through what is going on and notice he isn’t putting out any urine and that he has a massively distended abdomen.

Could he have abdominal compartment syndrome?
Abdominal compartment syndrome, the lesser known ACS, is defined as intra-abdominal pressure > 20mmHG. How do you find out the pressure inside the abdomen!?!?! Stryker needle the belly? I wish. Instead, you can use the foley to measure bladder pressure as a surrogate – details below.
You need to have a high clinical suspicion for ACS because these patients are critically ill, their exam is unreliable and imaging is not helpful.
Who gets abdominal compartment syndrome? Critically ill patients who have trauma, burns, massive ascites or intraperitoneal bleeding, ruptured AAA, pancreatitis or even that critically ill septic patient who got massively fluid resuscitated.
Why care? ACS can cause major problems for all of your organs and can ruin all your efforts to resuscitate your already critically ill patient. ACS can decrease cardiac output, increase peak inspiratory and mean airway pressures making them difficult to ventilate, cause anuria because of decreased kidney perfusion, and obstruct mesenteric blood flow causing gut ischemia to name a few.
What do you do if you have a patient with ACS? Surgical decompression! In the mean time you can place an NG and rectal tube to temporize. Place the patient supine to lower intraabdominal pressure. Avoid grossly overloading the patient with fluids. Optimize hemodynamics. If the patient has tense ascites you can perform a paracentesis. In the case of a burn victim, you can perform and escarotomy.
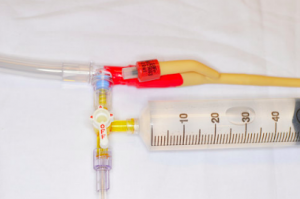
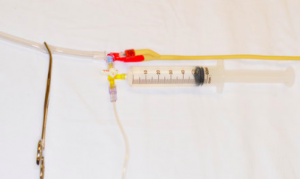
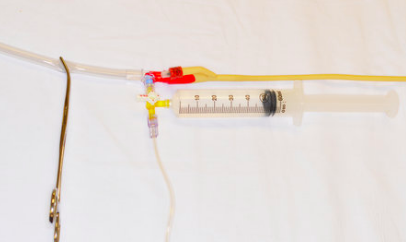
Measuring bladder pressure in the ED:
- Insert a Foley catheter and allow drainage of urine.
- Prepare a standard arterial line set-up and prime it using the 1 L bag of saline.
- Connect a stopcock attached to a 60 mL syringe of saline to the end of the arterial line tubing.
- Lie patient flat.
- Clean Foley catheter access port with an alcohol swab.
- Connect the three-way stopcock to the Foley catheter access port.
- Zero the pressure transducer at the level of the iliac crest in the mid-axillary line.
- Clamp the drainage bag of the Foley catheter just distal to the culture aspiration port using the Kelly forceps.
- Instill 60 mL of sterile saline into the bladder via the stopcock. Turn the stopcock off to the syringe and open to the patient upon completion of this.
- Briefly unclamp the distal Foley to allow all air in the proximal collection tubing to pass into the distal tubing, then reclamp.
- Allow 60 seconds for detrusor muscle relaxation prior to obtaining measurements.
- The bladder pressure should be taken at end-exhalation with the patient completely flat in the supine position. Ensure a good waveform prior to recording the measurement.
- Unclamp Foley when complete and remove pressure transducing tubing. If strict measurement of urine output is necessary for the patient, subtract 60 mL from the total urine output.

Want to learn more?
https://lifeinthefastlane.com/ccc/abdominal-compartment-syndrome/
http://www.emdocs.net/abdominal-compartment-syndrome-when-should-it-be-on-your-differential/
http://www.tamingthesru.com/blog/annals-of-b-pod/june-2017/abdominal-compartment-syndrome
Harrisson SE, et al, “Abdominal compartment syndrome: an emergency department perspective,” Emerg Med J, 2008.
Or check out the World Society of Abdominal Compartment Syndrome’s website: http://www.wsacs.org/ Yup, that’s real!
