aVR is the neglected cousin of the other ECG leads. He doesn’t always make sense, nobody really understands him, and he usually sits alone at the dinner table. This is to the detriment of those who ignore him, as aVR can easily lead clinicians down the correct clinical pathway if used correctly.
There are several morphologies of aVR which are very suggestive of certain conditions. You’ll find some examples below:
STE in Left Main Coronary Artery Occlusion
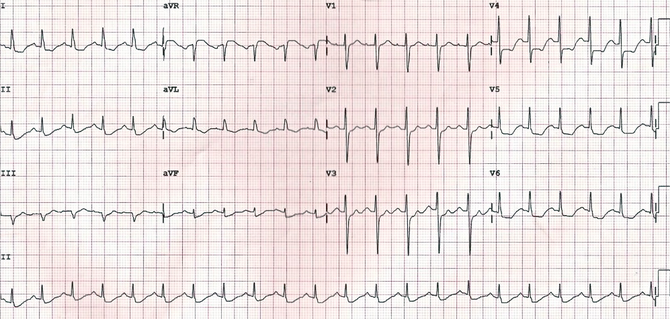
Courtesy of Life in the Fast Lane Blog (originally posted by Johnson Francis at Cardiophile.org)
Various studies were done to assess the utility of identifying STE’s in aVR. The largest study showed that a >0.05mV (0.5mm) ST elevation in aVR had a sensitivity of 78%, a specificity of 86%, a positive predictive value of 57%, and a negative predictive value of 95% for left main coronary artery occlusion. aVR is also useful in prognosticating. The odds ratio for death with STE’s > 0.05 and 0.1mV was 4.2 and 6.6, respectively. STE’s in aVR were shown to be an independent predictor of mortality.
PR Elevation and ST Depression in Acute Pericarditis
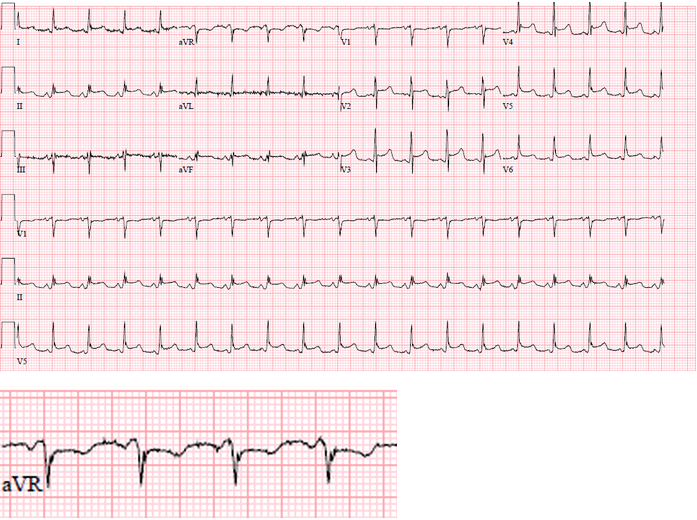
This is an ECG performed an a gentleman with acute bacterial pericarditis who developed tamponade. In aVR you can see both PR elevation and ST Depressions (see enlarged). Additionally, you see diffuse ST elevations in most other leads. The aVR findings in this case are suggestive of subepicardial atrial injury secondary to pericardial inflammation.
Enlarged R wave for TCA (and other sodium channel blockers) overdose
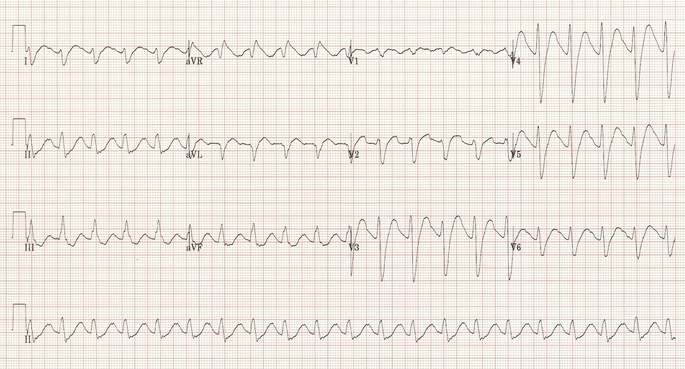
Courtesy of Life in the Fast Lane Blog
In addition to the other ECG findings for TCA overdose (sinus tachycardia, QRS widening, right axis deviation), an enlarged R wave in aVR is highly suggestive of cardiac and neurotoxicity. In one study, aVR height was directly proportional to severity of disease. For example, when comparing patients who experienced a seizure to those who did not in TCA overdose, the mean aVR height was 4.4mm in those who had a seizure in comparison to 1.8mm in those who did not. The R-to-S ratio was also found to be useful in predicting severity of disease, with a ratio of 0.7 or higher to be the ECG finding most strongly related to developing an arrhythmia (not QRS widening) with a PPV 41% and NPV 95% for the prediction of significant toxicity.
ST Elevations in aVR in SVT to Predict WPW
In one study of 338 patients who presented with supraventricular tachycardia (SVT), ST elevation in aVR was the only reliable finding on ECG that could be used to predict WPW (and other AV reciprocating tachycardias) from AVNRT and AT with a sensitivity of 71% and specificity of 70%.
Given these powerful findings, it’s important to keep aVR at the forefront of your ECG analysis because it can lead you to change management on some of your sickest patients.
For more information, see sources below.
Sources:
Williamson, A. Mattu, C.U. Pautz, A. Binder, W.J. Brady. Electrocardiographic applications of lead aVR. Am J Emerg Med, 24 (2006), p. 864
Burns E. Tricyclic Overdose (Sodium-Channel Blocker Toxicity). Life in the Fast Lane Blog. http://lifeinthefastlane.com/ecg-library/basics/tca-overdose. Accessed October 22, 2015.
Burns E. Abnormalities of the R Wave. Life in the Fast Lane Blog. http://lifeinthefastlane.com/ecg-library/basics/r-wave. Accessed October 22, 2015.
