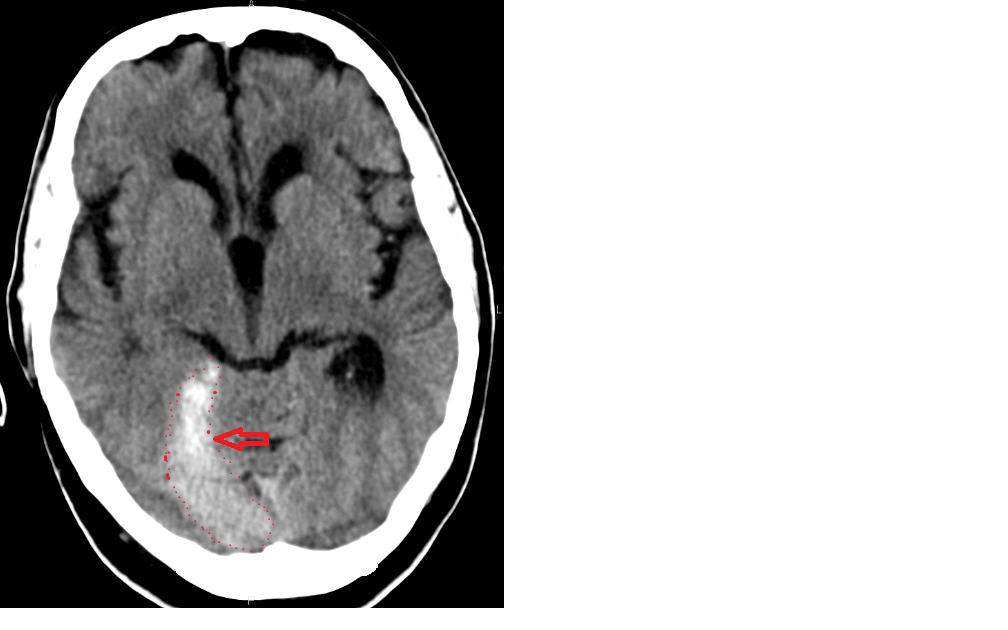
Tentorial/Peritentorial Subdural Hemorrhage – rare, but this is what they look like on CT. They may resemble intraparenchymal bleed on CT but MRI can confirm exact location with regard to the tentorium.
As a reminder, the tentorium is an extension of the dura; it separates the cerebellum from the inferior portion of the occipital lobes.

Subdural hematomas occur between the dura and arachnoid, in what is sometimes called a “potential space.” Subdurals are typically crescent-shaped, and fairly easy to identify with trauma to the calvarium. Further, they are usually more extensive than extradural hematomas. In contrast to extradural haemorrhage, SDH is not limited by sutures but are limited by dural reflections, such as the falx cerebri, tentorium, and falx cerebelli.
Although the mechanism responsible for traumatic tentorial SDH is still unclear, tearing of vessels adjacent to the tentorium (the bridging veins to the straight sinus or tentorial sinus) caused by linear brain acceleration during trauma is currently regarded as the most likely possibility. Takeuchi et al. looked at 32 cases of tentorial SDH and report that this mechanism is supported by finding 1) a high incidence of impact in the occipital or frontal regions and 2) a low incidence of skull fractures (31%).
Radiographically, tentorial subdurals are described as a “sheet-like area of increased attenuation with a sloping, hazy, lateral margin conforming to the general configuration of the tentorium, with a well-defined medial margin corresponding to the free edge of the tentorium.” MRI is useful when deciding whether neurosurgery can safely be performed to evacuate the blood. The optimal management strategy for tentorial SDHs is unclear, and studies are limited by the rare incidence of these cases. Takeuchi et al. posit that conservative therapy may be preferred if the patient’s neurological condition is stable, or if any accompanying diseases contraindicate surgery; however, surgery may be indicated for large bleeds or rapidly deteriorating mental status. All 32 cases in their paper were managed nonoperatively due to the small size of the bleeds.
Today’s Pearl is inspired by Lara Vanyo, who wrote that she “just had a patient with a story that could be convincing for subdural or intraparenchymal hemorrhage and had a CT which showed a subdural bleed along the tentorium which [she] totally thought looked like an intraparenchymal bleed.”
References
Govaert P, Calliauw L, Vanhaesebrouck P, Martens F, Barrilari A: On the management of neonatal tentorial damage. Eight case reports and a review of the literature. Acta Neurochir (Wien) 106: 52–64, 1990
Matsumoto K, Houri T, Yamaki T, Ueda S: Traumatic acute subdural hematoma localized on the superior surface of the tentorium cerebelli–two case reports. Neurol Med Chir (Tokyo) 36: 377–379, 1996
Takeuchi, S., Y. Takasato, H. Masaoka, et al. Traumatic peritentorial subdural hematomas: a study of 32 cases. Turk Neurosurg, 22 (2012), pp. 305–308
Images from Wikipedia and http://4.bp.blogspot.com/-UB-JyJXrBtc/UAL8wAWimPI/AAAAAAAABbw/ZpOr9c3HWkQ/s640/Lam+2.png
