
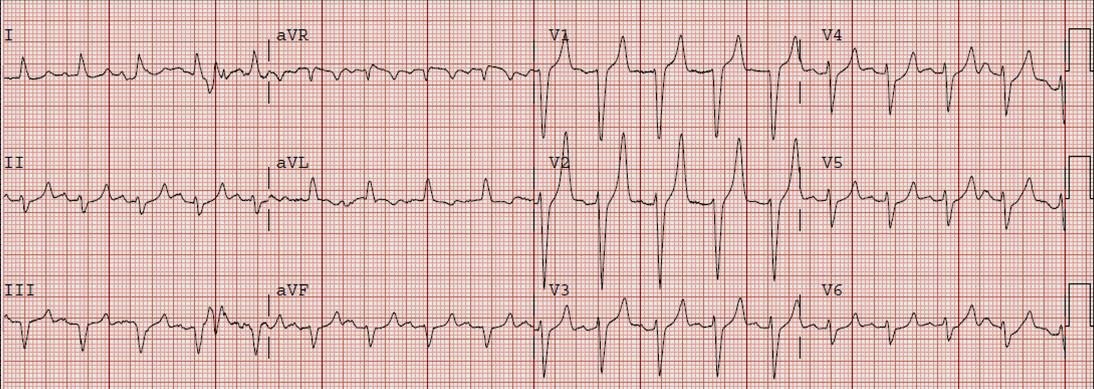

What do all these EKGs have in common? They are all hyperkalemia! How hyperK+ are they? Turns out it is probably hard to say…there’s a Basic Rubric:
- Peaked T waves K>5.5mEq/L
- Prolongation of PR interval/loss of P wave K> 6.5mEq/L
- Widening QRS Complex K>7.omEq/L
- “Sine Wave”/Interventricular conduction Abnormalities/Asystole K>9.0mEq/L
But a lot of the data (ALiEM QI Series: Pitfalls in Diagnosing Hyperkalemia) says if you see any of this you should be concerned therefore what do you reach for first? [Review Weingart’s podcast!]
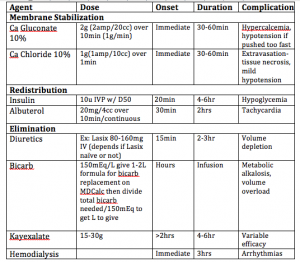
- Therapies for HyperK+ [adapted from Weisberg 2008 table]
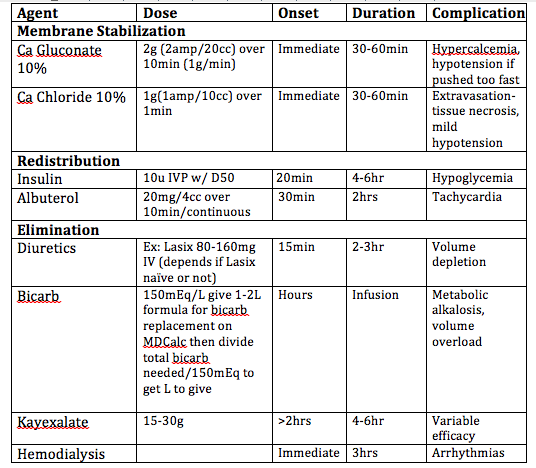
- Grab CaCl vs CaGluconate- What you choose may in part be based on:
- IV access central line vs peripheral: Central line definitely use CaCl Why?
- CaCl works quickly you can push it over approx 1 min as opposed to CaGluconate that needs to be infused over approx 10min to prevent hypotension (2/2 large sugar moeity-gluconate)
- Also 1g CaCl=3g CaGluconate
- Bioavailability? Actually studies have shown that both Cl and gluconate have similar concentrations in the blood within the same timeframe indicating CaGluconate may not need to undergo hepatic metabolism before becoming active
- Clinical Status-patient looks like they are not long for this world: Use CaCl for all the reasons above even if they have a peripheral-ideally large 18g in the AC (risk of extravasation is lower than risk of life lost)
- IV access central line vs peripheral: Central line definitely use CaCl Why?
- Now the cardiac membrane is stabilized or is it…?
- Repeat EKG better? worse? same? may need to repeat CaCl vs CaGluconate if no effect within a few minutes and patient still looks bad
- Redistribute the K+
- Insulin 10u/D50: pushes K+ back into cells
- Albuterol 20mg (continuous nebs): pushes K+ back into cells
- Eliminate the K+
- Diuretics: Lasix 80-160mg and others…see PulmCrit for more!
- IV Bicarb: 150mEq/L-probably give 1-2L but formula on MDCalc find out bicarb deficit then divide/150mEq to get liters needed to give
- Eliminates K +by (1) driving K+ back into cells (2) Eliminating K+ through renal excretion (3) dilutional effect on K+ check out PulmCrit for more!
- Kayexalate: not as effective in emergent management but consultants will want it; as indicated on chart takes >2hrs to onset! (hopefully patient is in ICU by now but reality is they may not be)
- Hemodialysis: place Shiley dialysis catheter preferably Trialysis (triple lumen) Catheter (Call MICU)-good time to check catheter placement as it is a big catheter and want to make sure you’re not cannulating the wrong vessel see Milliner’s pro lineman Pearl
- IVF controversial NS may not be ideal bc it may induce hyperchloremic metabolic acidosis may want to opt for LR (even though it has K+) or discuss with team see PulmCrit for more!
Mnemonic KHALEESI for remembering HyperK management
K-Kalcium-CaCl or Ca Gluconate/Kayexalate prob for upstairs mgmt
H-H+ acidosis correct w/ Bicarb 150mEq/L
A-Albuterol give 20mg continuous nebs
L-Leads EKG needed to make sure therapy is effective
EE-Eliminate/Excrete K+ via Diuretics like Lasix, Kayexalate for upstairs
S-Shiley may be needed for dialysis
I-Insulin 10u IV/D50 to prevent hypoglycemia
Sources:
- Hyperkalemia. 2016. http://lifeinthefastlane.com/ecg-library/basics/hyperkalaemia/
- Polevoi, S. 2013. ALiEM QI Series: Pitfalls in Diagnosing Hyperkalemia. https://www.aliem.com/2013/qi-series-hyperkalemia/
- Weingart, S. 2010. EMCrit Podcast 32 – Treatment of Severe Hyperkalemia. http://emcrit.org/podcasts/hyperkalemia/
- Hayes, B. 2013. Mythbuster: Calcium Gluconate Raises Serum Calcium as Quickly as Calcium Chloride. https://www.aliem.com/2013/mythbuster-calcium-gluconate-raises-serum-calcium-as-calcium-chloride/
- Weisberg, L. 2008. Management of severe hyperkalemia. Critical Care Medicine. 36(12):3246-3251
- Farkas, J. 2015. Management of severe hyperkalemia in the post-Kayexalate era. http://emcrit.org/pulmcrit/management-of-severe-hyperkalemia-in-the-post-kayexalate-era/
