In light of this morning’s toilet-related malfunction and Noah’s Ark-like flooding of the PA Conference Room……here are a few quick-to-read pearls about the drowning patient.
Epidemiology
- Leading cause of death worldwide among boys 5 to 15 years of age
Risk Factors
- male sex (yeah, we do dumb things)
- age < 14
- alcohol use
- low income
- poor education
- rural
- lack of supervision
- epilepsy (15-19x higher risk)
Definition
- “Process of experiencing respiratory impairment from submersion/immersion in liquid” (WHO, 2002)
Process
- Airway goes below surface (submersion) or water splashes over face (immersion) -> patient cannot keep airway clear -> water entering mouth is spat out or swallowed -> breath holding (~ 1 min) -> some water aspirated into airway -> coughing reflex -> laryngospasm -> aspiration continues -> hypoxemia -> loss of consciousness and apnea -> tachycardia to bradycardia to PEA to asystole
- Water in alveoli causes surfactant dysfunction, atelectasis, V/Q mismatch, ARDS
Pre-Hospital Pearls
- Cardiac arrest primarily due to lack of oxygen. Thus, start with 5 initial rescue breaths (water in airways can interfere with effective alveolar expansion), 30 compressions, then continue with 2-to-30 ratio. A-B-C, not C-A-B.
- If unconscious, in-water resuscitation improves likelihood of favorable outcome
- Ventilation alone, as compressions futile in deep water
- With respiratory arrest, there is usually a response after a few rescue breaths
- If no response, assume cardiac arrest and bring to dry land for CPR
- While bringing to dry land, try to maintain vertical position with airway open to prevent vomiting and aspiration
- If no response, assume cardiac arrest and bring to dry land for CPR
- If unconscious but breathing, put in lateral decubitus position
ED Pearls
- Most critical prognosticator is duration of submersion
- A-B-C, not C-A-B (as above).
- Cardiac arrest usually due to hypoxemia. May correct with improved oxygenation.
- Routine C-spine immobilization can interfere with airway management and is not recommended unless clinically indicated based on events.
- Goal of hospital management: prevent secondary neurologic injuries due to ongoing ischemia, cerebral edema, hypoxemia, fluid and electrolyte imbalances, acidosis, and seizure activity
- Early intubation and mechanical ventilation (ARDS guidelines, i.e. PEEP) if indicated
- Indications: neurologic deterioration, need to protect airway, unable to maintain PaO2 >60 mmHg or O2 sat >90 despite high-flow O2, PaCO2 >50
- Keep ventilated for at least 24 hrs before attempting to wean; minimize recurrence of pulmonary edema and reintubation
- Permanent neurologic damage is the most worrisome outcome
- Hypothermia may slow this process
- Healthy individuals with spontaneous respirations, clear breath sounds, and an O2 sat >90% with no focal neurologic deficits may need only temporary supplemental O2 or no treatment at all prior to discharge
- Volume of fluid aspirated in most immersions is only 3 mL/kg, not enough to cause significant hemodynamic and electrolyte abnormalities. In other words, saltwater versus freshwater immersion no longer considered significant.
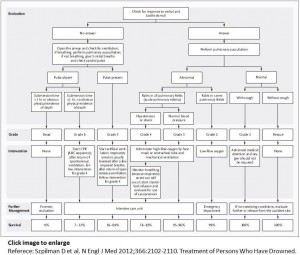
- MANAGEMENT ALGORITHM

Poor Prognosticators
- Duration of submersion > 5 min
- Time to BLS > 10 min
- Resus duration > 25 min
- Age > 14
- GCS < 5
- Persistent apnea and requirement of CPR in ED
- ABG pH < 7.1 on presentation
References
Chandy D, Weinhouse G. Drowning (submersion injuries). UpToDate April 2015.
Meisenheimer E, Bevis Z, Tagawa C, Glorioso J. Drowning Injuries: An Update on Terminology, Environmental Factors and Management. Current Sports Medicine Reports. March/April 2016, 91-93.
Schmidt A, Sempsrott J, Havryliuk T, Semple-Hess J. Drowning in the Adult Population: Emergency Department Resuscitation and Treatment. Emerg Med Pract. 2015 May;17(5):1-20.
Szpilman D, et al. Treatment of Persons Who Have Drowned N Engl J Med 2012;366:2102-2110.
