Overdose and EKGs they start to all look the same…widened QRS, that thing in aVR…vfib (hopefully not). Here’s a highlight of key EKG findings associated with a few toxidromes: (1) Bupropion overdose (2) TCA overdose (3) Digoxin Toxicity
Bupropion Overdose:
- See wide-complex tachydysrhythmias-widened QRS and QT intervals; case reports have shown cardiogenic shock
- Consider in the patient who is seizing and was trying to quit smoking (primarily used for nicotine suppression)
- See seizures approx. 2-8hrs after toxic ingestion but can see up to 24hrs later
- May try NaHCO3 but probably will not work, mainstay for therapy is supportive care
TCA Overdose:
- QRS widening >100ms associated with seizures; >160ms associated w/ cardiac dysrhythmias
- Terminal R wave >3mm in aVR
- R/S ratio >0.7 in aVR
- RBBB pattern
- Tachy
- Can also see sedation, seizures, hypotension…
- Management includes NaHCO3 increases amount of non-ionized form and decrease binding to Na channels
- Scott Weingart’s target: QRS duration <100, hemodynamically stable, Na ~150, pH ~7.5
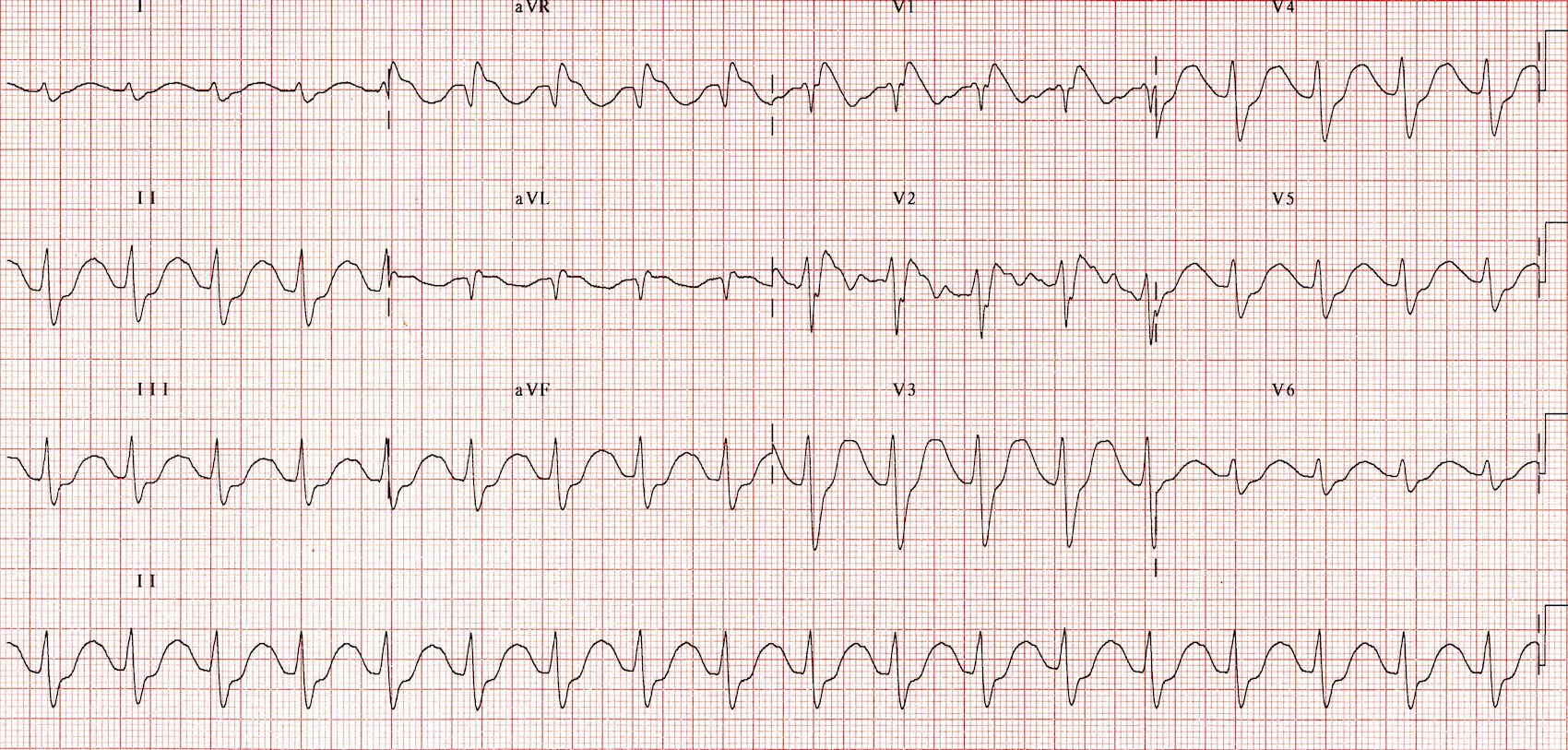
Digoxin Toxicity
- Chronic toxicity usually found in the elderly and those patient w/ renal impairment
- AV nodal block, Bradycardia, tachyarrhythmias-junctional tachy, atrial tachy, ventricular ectopia
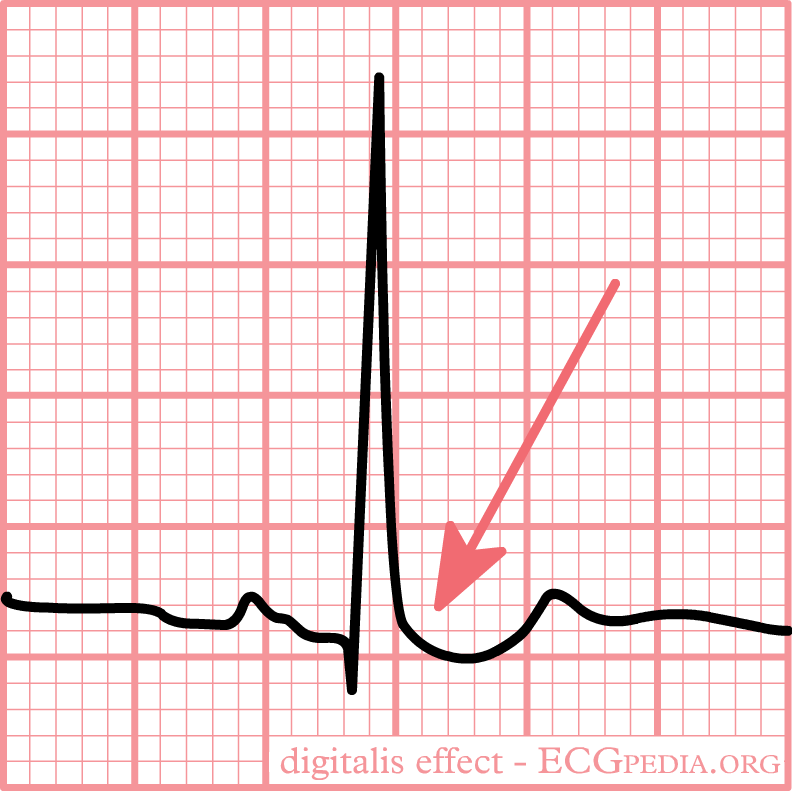
- ST-T segment has a scooped appearance like “Salvador Dali’s mustache” or “reverse check mark”
- GI distress, hyperkalemia
- Tx: Digibind for: cardiac arrest, life-threatening dysrhythmias, K>5mmol, >10mg ingested (adult), >4mg ingested, Dig level >12ng/ml
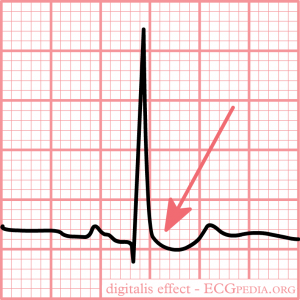
- ECGPedia.org/”Salavador Dali mustache” aka “reverse check mark sign”
Manini et al 2010 Reviewed EKG findings in suspected acute poisoning and the incidence of adverse cardiovascular events (ACVE) and found that non-sinus rhythm, prolonged QTc, ventricular ectopy, QT dispersion (QT interval minus minimum QT interval in different leads), and presence of ischemia correlated w/ risk of ACVE.

RECAP:
- Bupropion toxicity-widened QRS, seizures probably not responsive to NaHCO3
- TCA Toxicity-terminal R in aVR, widened QRS, tachyarrhythmias, RBBB, hopefully responds to NaHCO3
- Digoxin-“reverse check mark sign”/”Salvador Dali mustache”-ST-T segment scooping, AV nodal block
- Manini et al 2010 suggested key findings such as prolonged QTc and non-sinus rhythm as findings associated w/ adverse cardiac events
Sources:
- Bupropion. http://lifeinthefastlane.com/tox-library/toxicant/anti-depressants/bupropion/
- Weingart, S. Podcast 98. Cyclic (Tricyclic) Antidepressants Overdose
- Digoxin Toxicity. 2014. http://lifeinthefastlane.com/ccc/digoxin-toxicity/
- Manini, A. F., Nelson, L. S., Skolnick, A. H., Slater, W., & Hoffman, R. S. (2010). Electrocardiographic predictors of adverse cardiovascular events in suspected poisoning. Journal of Medical Toxicology, 6(2), 106-115.
