Intro:
You are at Elmhurst and it’s your first cardiac shift ever. EMS rolls in, “Hey Doc, this patient is in a-fib.” The patient’s heart is beating fast. Your heart is beating fast.
He is a 70 year old patient with a PMH of HTN, CKD, and COPD presenting from the nursing home with SOB. Patient is normotensive, altered, febrile, tachypneic, tachycardic to 130s, and hypoxic to high 80s on a NRB. Code status: DNR/DNI. What do you do?
tl;dr: Story Time (<5 minutes)
Ok so it wasn’t my first ever cardiac shift. We placed the patient on BIPAP immediately. The 12 lead EKG was ordered and consistent with a-fib rvr. POCUS showed a collapsible IVC with adequate EF and no b-lines. Sepsis protocol was initiated. We got labs, gave fluids and abx. CXR was concerning for possible pneumonia. I (unsuccessfully) attempted to call family members and the health care proxy. In other words: patient was stable-y unstable. Ultimately the patient was admitted to medicine step down and was boarding in the ED. We’re done, right?
A few hours later transport came to take the patient upstairs. But of course, BP now on monitor is 70s systolic with a HR in the 160s. Do I shock this patient who is now unstable with a-fib rvr? He is DNR, but technically has a pulse. Did anyone explicitly consent for electricity in their code discussions? I had recognized that the a-fib was driven by sepsis and had attempted to adequately resuscitate him…but now he’s crumping. What should I do now?
Naturally Ram came to the rescue. He asks for a phenylephrine stick and gives 200 mcg. I see the next two BPs improve to 150s systolic with a HR in the 150s. We then push 20mg of IV Diltiazem and voila: HR in the 120s. I fixed him….well, Ram fixed him.
Phenylephrine is a pure alpha agonist. This supports the patient’s blood pressure with the added benefit of some reflex bradycardia via the carotid baroreflex. Norepi and epi are generally avoided in the hypotensive a-fib rvr patient as they also have beta agonist activity and can increase the HR further in these patients.
Truly fascinating. I spoke to Kunj, who said he did it once. Micah Nite said he does this all the time. Eventually transport came back and took the patient upstairs. I take that dispo as a win.
Keep reading if you wanna learn more.
Extended Pearls – (>5 minutes)
A-fib: Caused by multiple atrial microentery circuits causing unorganized depolarization and atrial contractions. Ultimately reduces cardiac output by reducing diastolic filling and decreases ventricular stroke volume. Over time there is atrial remodeling from chronically sustained tachycardia leading to altered expression and function of cardiac ion channels.
EKG: Narrow complex irregularly irregular EKG. No P wave before every QRS. No QRS after P waves. Average HR is around 120-180s.
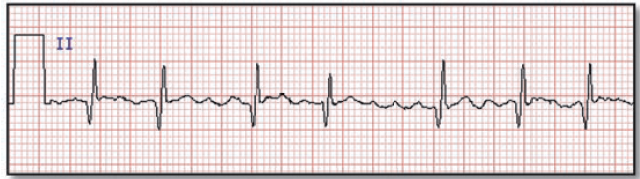
Look at this chaotic electrical activity. Absent P-waves. Irregularly irregular ventricular response. CHAOS.
(WPW on the other hand is often wide, fast, and irregular. If HR > 200 consider WPW. Also don’t confuse it with a-flutter which can have some regularity or Multifocal Atrial Tachycardia (MAT) that has p-waves with different morphologies.)
Common causes of new onset A-Fib:
| A | Alcohol Abuse – Holiday heart syndrome |
|---|---|
| T | Thyroid Disease |
| R | Rheumatic Heart Disease |
| I | Ischemic Heart Disease |
| A | Atrial Myxoma, myopathy, mitral valve disease included |
| L | Lung – PE, PNA, COPD, hypoxemia |
| F | (Ph)eochromocytoma, Fluid status |
| I | Infection/sepsis |
| B | Blood Pressure – HTN, Beta agonists – norepi, epi, dobutamine |
Management: Often, treating the underlying condition that is stimulating the patient’s sympathetic drive pushing them into a-fib is necessary. Treating a-fib with medical management or cardioversion may not be effective if you do not treat the underlying cause.
Treatment: Determine if the patient is stable vs unstable. Delineate if the instability is being driven by another cause (sepsis, PE, etc) or if the a-fib is driving the instability.
If unstable (hypotensive, hypoxic, decreased responsiveness): synchronized electrical cardioversion with 200 J.
Oftentimes patients may need the compensatory tachycardia to maintain cardiac output. If HR > 150 the patient likely has impaired cardiac diastolic filling and should be treated appropriately. Some patients may be asymptomatic and are able to tolerate higher HRs. However patients that rely on their atrial kick (mitral stenosis, pulmonary htn, diastolic HF) will not be able to tolerate higher HRs.
So how do you decide if you want to rate vs. rhythm control? Studies have shown no mortality benefit or stroke benefit in choosing rate vs. rhythm control.
Commonly used AV nodal blocking agents for rate control with target HR around 120-130:
| Drug | Loading Dose | Maintenance Dose |
| Metoprolol | 2.5-5mg IV over 2 minsRepeat every 5 min up to 15mg total | 25-50mg PO, lasts 12 hours |
| Diltiazem (weight based dosing) | 0.25mg/kg, repeat 0.35mg/kg. Average dose is 10-20mg IV over 2 mins. | 30mg PO, redose every 6 hours |
There are many other antidysrhythmic drugs that can be used which are not discussed here.
If the HR is not responsive to the first dose of IV medication, give another one. IV meds need to be chased with PO medication otherwise the patient will just go back into a-fib rvr. The patient’s heart will beat fast again. Your heart will beat fast. It is a toxic cycle.
Important to note these medications should not be used in patients with WPW. Blocking the AV node conduction with retrograde conduction into the accessory pathway can accelerate the ventricular rate, potentially pushing the patient into V-fib.
Choosing the right medication: This depends on the patient’s underlying medical condition. If the patient has known history of a-fib you can always give them their home medication. For rate controlling new onset a-fib, calcium channel blockers (Diltiazem) should be favored over beta blockers in patients with asthma. While commonly beta blockers (such as Metoprolol) are given in thyrotoxicosis.
Both calcium channel blockers and beta blockers can cause hypotension. This is where phenylephrine comes in.
Phenylephrine: Is a pure alpha agonist. This supports the patient’s blood pressure with the added benefit of some reflex bradycardia via the carotid baroreflex. But Mariam, won’t this decrease the patient’s cardiac output?! Well emcrit does a beautiful job explaining this: phenylephrine essentially has variable effects on cardiac output. Reflex bradycardia and arterial constriction can decrease cardiac output; however, venoconstriction increases cardiac output by increasing preload. Norepinephrine and epinephrine are generally avoided in the hypotensive a-fib rvr patient as they have beta agonist activity and can increase the HR further.
Phenyl sticks are readily available in the Elmhurst cardiac room and in resus at Sinai. Push dose phenyl comes as 1,000 mcg/10mL or 100mcg/mL. Push 1-2 cc at a time until you get the desired BP.
Rhythm control (v quick summary):
Electrical cardioversion: Cardioversion has a high success rate for rhythm control when a-fib has been present for less than 48 hours. Risk of thromboembolism increases with cardioversion the longer the patient has been in a-fib.
Chemical cardioversion: Many drugs including amiodarone can be used to convert patients from a-fib to sinus rhythm. This again poses a risk of thromboembolic events if a patient has been in a-fib for longer than 48 hours similarly to electrical cardioversion.
Catheter ablation: Can lead to return of sinus rhythm and eliminate the need for prolonged medical therapy.
Anticoagulation: Development of left atrial thrombi in patients with a-fib can cause embolic events leading to a 5 fold increased risk of stroke in these patients. The CHA2DS2VASC score is a point based risk stratification system that can be used to guide anticoagulation initiation. Look it up on MDCALC!
Disposition:
- New onset A-fib: patient often requires admission for further workup including cardiology eval, TTE or continued management of sepsis/electrolyte/metabolic abnormalities.
- Discharge? Potentially an option for the patient with known a-fib, already on home meds who is no longer in a-fib rvr and has close outpatient follow-up.
Further Resources
BCC: Episode 114 – Atrial Fibrillation https://emcrit.org/ibcc/af/
FOAMcast: atrial fibrillation/flutter
Rosen’s – Chapter 69: Dysrhythmias, 9th edition
