tl;dr – Story Time (<5 minutes)
Patient is a 59 year old MTF with a PMH of HIV (undetectable viral load) and HTN (on amlodipine) BIBEMS for evaluation of “pinching” chest pain and right flank pain. EKG in triage revealed sinus bradycardia – HR 55 with a BP 130/70s. Patient was well appearing, endorsed chest pain that resolved but was still having right flank and now thigh pain. Patient was presented to the cardiac room, orders were placed to expedite work up, and was deemed stable for the side…
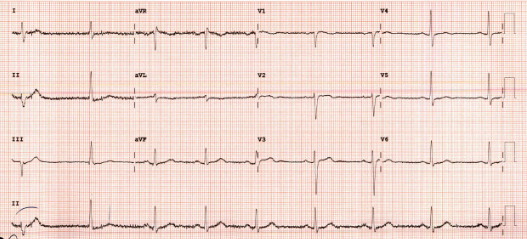
EKG: Sinus bradycardia without STE, STD, or TWI. No prior ekg available.
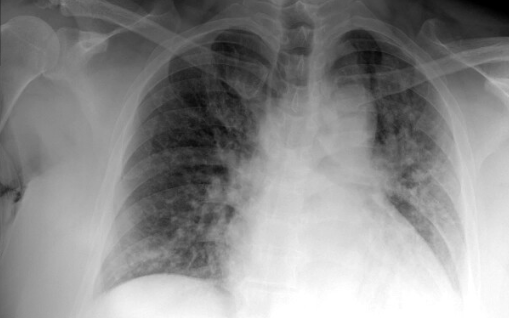
In the ED patient was given pain medication, electrolytes were within normal limits, BNP 136, Troponin negative. CXR was concerning for mild pulmonary congestion. Something was not adding up. A d-dimer was added on (our thinking was chest pain with leg pain, maybe this is a PE?) and was elevated at 2,694. I signed out this patient pending CTA. CT angio was done and initially read as negative.
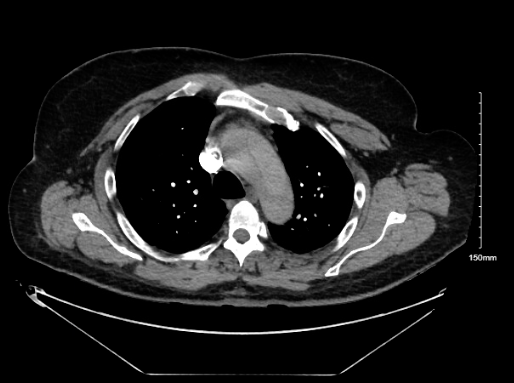
Fast forward…the patient became hypotensive, tachycardic, and altered a few hours later. They were upgraded to the cardiac room. POCUS revealed a moderate pericardial effusion and an aortic flap concerning for aortic dissection. CT angio read was now edited and read as an aortic dissection. Surgery was consulted. Sinai accepted the patient for transfer.
Shortly after EMS arrived, the patient lost pulses and coded. Patient was quickly intubated by Dr. Potter. POCUS revealed signs of tamponade and a pericardiocentesis was performed by the one and only Dr. Puja Patel with removal of 5cc of clotted blood. Unfortunately the ED team was unable to obtain ROSC and the patient expired.
This is a commonly missed and devastating diagnosis with a high mortality rate. Pain that is not described as “tearing” or “ripping” should not make you exclude the diagnosis. Ultimately, I learned that we needed to have a higher clinical suspicion for aortic dissection in patients with “chest pain and…” symptoms.
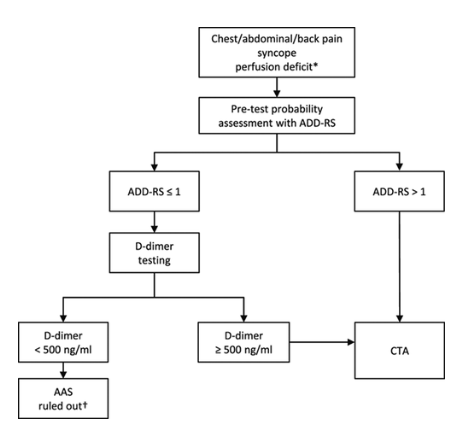
My question to you: Should we be using a more standardized approach to rule out dissection such as ADD-RS (sensitivity of 98.8% in patients with a score of 0 or 1 and a negative D-dimer)?
Keep reading if you want to learn more.
Extended Pearls – (>5 minutes)
Aortic dissection: Caused by a tear in the intima that causes blood to dissect through the aortic media, creating a false lumen. It Is a rare, commonly missed, and life threatening diagnosis (mortality rate 27% with 1%/hr after onset).
Presentation: Often the presentation is very broad and variable given that it is a dynamic process (the tear can occur anywhere along the aorta and extend). The International Registry of Acute Aortic dissection (IRAD) published a study in 2000 revealing only 73% of patients present with complaints of chest pain, 85% have sudden onset pain, and 4% are pain free. Think about aortic dissection in patients with chest pain plus symptoms including symptoms above and below the diaphragm- extremity pain, migratory pain, syncope, back/abdominal pain, or new neurological deficits.
Risk factors: HTN (chronic shearing force of blood into aorta causes medial degeneration), age, prior hx of dissection, aneurysm, crack/cocaine use, connective tissue disorders, recent CATH/cardiovascular surgeries, arteritis, structural abnormalities, syphilis, etc
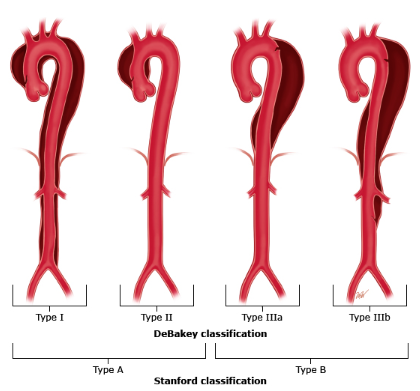
Classification: We commonly use the Stanford criteria that is based on the anatomical position where the dissection originated: Type A and Type B. Stanford Type A involves the proximal ascending aorta and requires surgery. Aortic regurgitation in Type A dissections can present as congestive heart failure. Type B dissections include only the descending aorta, distal to the left subclavian artery and can be medically managed.
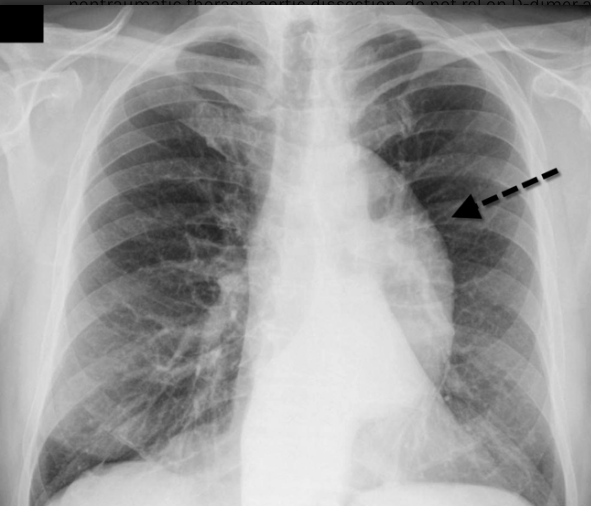
Imaging: EKG could have no abnormalities (31% of cases) or show signs of ischemia (3-5% of cases) due to proximal dissection into the coronaries. CXR can reveal a wide mediastinum (61% of cases) or be completely normal. POCUS of the suprasternal notch to view the proximal aorta and abdominal aorta can be done which would reveal a dissection flap (low sensitivity, high specificity). CTA is 100% sensitive and 98% specific for aortic dissection.
“Double Rule Out”: A CT-PE study is done at an earlier phase to optimize contrast in the pulmonary artery vs. a dissection study that is done at a later phase to visualize the aortic root, requiring more contrast and radiation to view the entire aorta. A CT-dissection study can often catch a PE while a PE-study will often miss a dissection. This is because a CT-PE study will always be too early to adequately visualize the aorta. However a CT-dissection study may visualize the pulmonary artery if there is still residual contrast being injected. Call your radiologist to discuss the study and let them know both are on the differential so they can attempt to modify the dissection protocol for a double rule out scan.

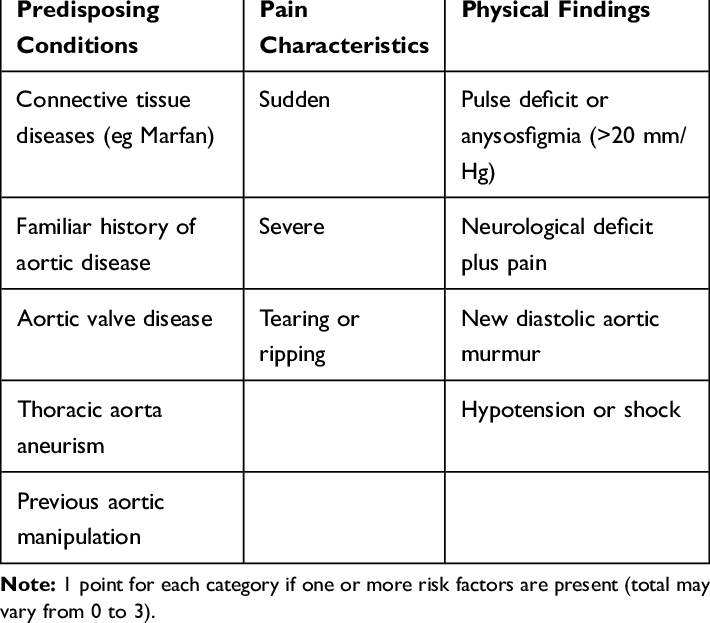
Aortic Dissection Detection Risk Score (ADD-RS tool): The ADvISED trial was a multicenter prospective observational study published in 2018 that studied a standardized approach to rule out aortic dissection using the ADD-RS tool in combination with a D-dimer test.
The ADD-RS tool consists of 12 clinical risk markers identified by the American Heart Association (AHA) and the American College of Cardiology (ACC) in 2010. Patients are given a score of 0-3 based on predisposing conditions, pain characteristics and physical findings. A D-dimer should be considered to risk stratify if the patient has a score of 1 or below while a CTA should be considered in patients with a score greater than 1. The ADvISED trial revealed that an ADD-RS of 0 or 1 with a negative D-dimer had a sensitivity of 98.8% in ruling out aortic dissection.
Disclaimer: The detection risk score is not externally validated even though the original trial was observational and has limitations. Fill out this quick poll and let me know what you think!
Management: So you caught an aortic dissection, what do you do now?
1. Pain control: Imagine the feeling of your aorta ripping in your chest. Treat your patient’s pain!
2. HR < 60: Control HR before blood pressure to prevent reflex tachycardia, which will result in increased aortic wall stress.
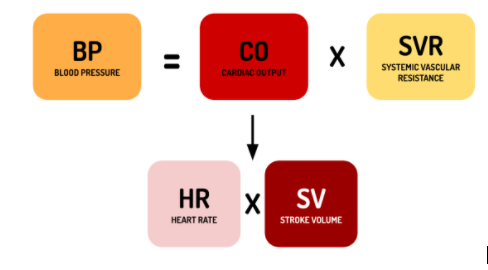
3. SBP < 120: BP should be controlled to decrease shearing forces on the intima and prevent extension of the dissection.
| Fentanyl | Bolus and gtt |
| EsmololHR <60 | 500 mcg/kg over 1 min Gtt at 50-300 mcg/kg/min (titrate by 25 mcg/kg/min q5min) |
| Nicardipine SBP < 120 | 5-15 mg/hr (start at 5 and titrate by 2.5 mg/hr q5mins |
4. Reverse AC if present.
5. Consult surgery early and transfer to a site with cardiothoracic surgery.
Quick tl;ldr on cardiac tamponade: The hypotensive patient with an aortic dissection likely has cardiac tamponade secondary to the dissection progressing to the pericardium or hypovolemia due to adventitia rupture. Briefly, POCUS can be used to differentiate a pericardial effusion that is causing clinical decompensation. POCUS findings: right atrial collapse during systole, right ventricular collapse during diastole, respiratory flow variation across mitral valve, and distended IVC (pointing to an obstructive shock pattern).
Further Resources:
Rosens Chapter 75 – Aortic Dissection
https://www.emrap.org/corependium/chapter/recN9AXGWMstEm8CO/Aortic-Dissection#h.fagqh9cjf90g
http://www.emdocs.net/acute-aortic-dissection-3/
