Trauma is the leading cause of non-obstetric death in pregnant women. MVAs and intimate partner violence account for most cases.
Let’s first discuss the physiological changes to consider when managing a pregnant patient in a trauma.
- AIRWAY:
- Progesterone: floppier airway with more edema
- Predict a more difficult tube
- Decreased esophageal tone and -> higher risk for aspiration
- Decompress early with NG or OG tube
- Progesterone: floppier airway with more edema
- BREATHING:
- Increase in respiratory drive -> hyperventilation -> chronic respiratory alkalosis -> fall in bicarb
- Decrease in functional residual capacity due to upward displacement of diaphragm.
- Less reserve when intubating! Preoxygenation and apneic oxygenation are extra important.
- CIRCULATION:
- Cardiac output increases by up to 50%, due to increase in blood volume (increases preload), decrease in SVR (progesterone -> decreased afterload), and increase in HR.
- Vitals may not readily reflect significant blood loss.
- Replace volume liberally (O negative blood).
- Gravid uterus can compress the IVC and displace the diaphragm
- Position in left lateral decubitus
- Displace uterus to the left during compressions
- Chest tube 1-2 IC spaces above
- Cardiac output increases by up to 50%, due to increase in blood volume (increases preload), decrease in SVR (progesterone -> decreased afterload), and increase in HR.
Management:
- Fetal FAST: number of fetuses and position, placental location (exclude placenta previa before vaginal exam!), amniotic fluid volume, fetal cardiac activity, and femur length (> 4cm may survive ex-utero)
- Vaginal exam: look for bleeding, amniotic fluid, cervical dilation or effacement
- Immunization:
- Anti-D immune globulin for rhesus D negative patients
- Kleihauer-Betke: quantifies maternal-fetal hemorrhage to de
- Tetanus vaccine is safe in pregnancy
- Anti-D immune globulin for rhesus D negative patients
- Antenatal corticosteroids: typically viable 23 to 34 weeks gestation
- Don’t forget to screen for intimate partner violence
- Admit at least 24 hours: uterine tenderness, vaginal bleeding, contractions at least once every 10 minutes, rupture of membranes, abnormal FHR, high risk mechanism, hypofibrinogenemia
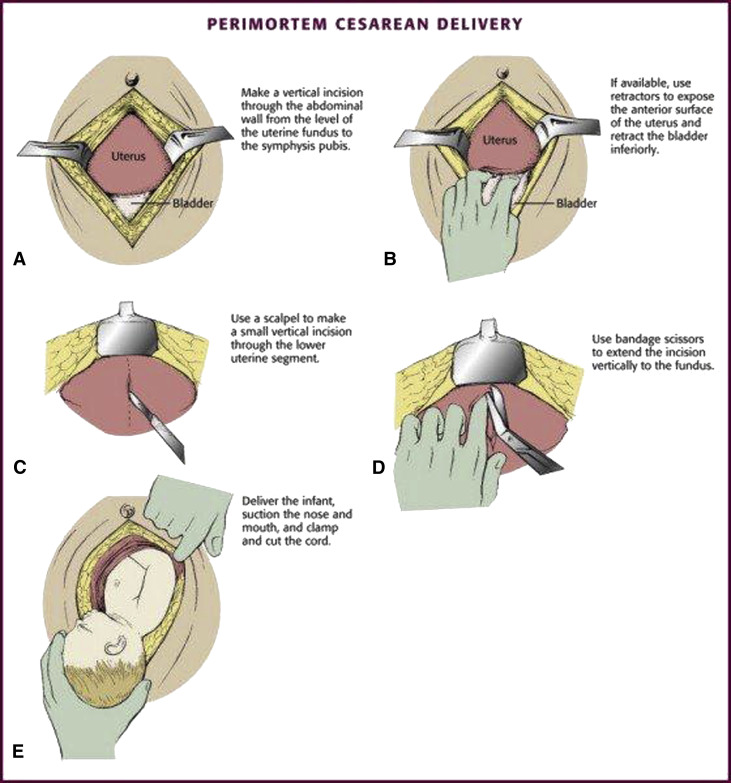
- Resuscitative hysterotomy aka Perimortem cesarean (> 24 wk): Initiate WITHIN FOUR MINUTES. Patient codes, no ROSC at first pulse check -> start gathering supplies for C-section. You mostly just need betadine, a 10-blade scalpel, and scissors. The thoracotomy tray also has everything you need (scissors, retractors, clamps).
- Call OB, Peds, NICU, Trauma, RT
- Primary benefit is saving mom’s life by both redirecting blood flow, reducing demand, and relieving pressure from the IVC and aorta
- Secondary benefit to deliver baby (the faster, the better chances)
- Prep neonatal resuscitation supplies, including warmer
Love, Julie
Resources:
https://www.uptodate.com/contents/initial-evaluation-and-management-of-major-trauma-in-pregnancy
https://www.jogc.com/article/S1701-2163(15)30232-2/pdf
https://www.ajog.org/article/s0002-9378(13)00068-9/fulltext
http://www.emdocs.net/resuscitation-of-the-pregnant-trauma-patient-pearls-pitfalls/
