Intraoral POCUS in the Management of Peritonsillar Abscess
Posted on by
Daniel Thomas
A peritonsillar abscess (PTA) is an abscess in the peritonsillar space between the tonsillar capsule, superior constrictor, and palatopharyngeus muscles.
If on your initial primary survey, you have concern for airway compromise: drooling, stridor, hypoxia, sniffing position, increased work of breathing, or tripoding–secure the airway. It may be a difficult intubation. Consider awake fiberoptic intubation if time permits, otherwise, dual setup for surgical airway while attempting intubation. And emergently consult ENT, give steroids, and antibiotics.
Assuming you have a patient who isn’t as critical as the above scenario, you want to keep it that way. You want to prevent airway compromise and systemic infection. Untreated complications include upper airway obstruction and airway compromise, mediastinitis, pericarditis, Lemierre’s syndrome, and carotid artery erosion causing fistula.
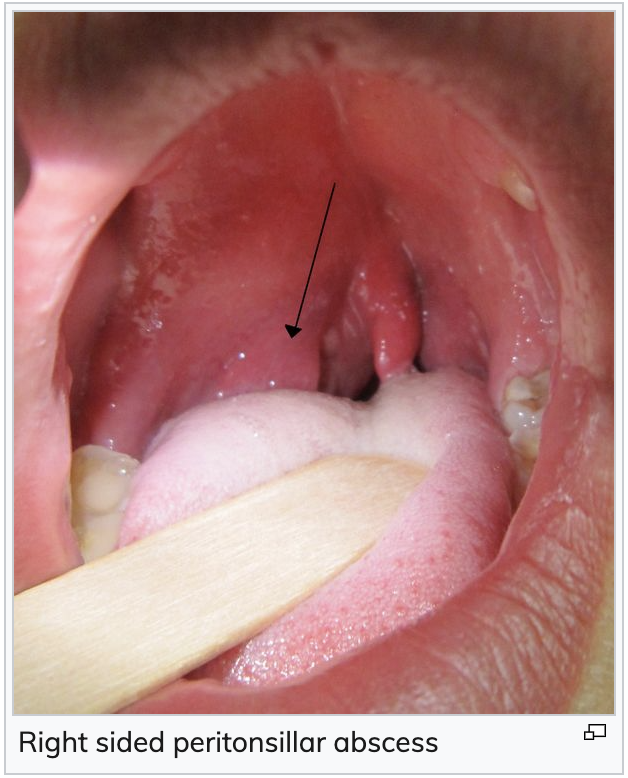
Classically, PTA presents with trismus, muffled voice, and unilateral peritonsillar swelling with displacement of uvula to the contralateral side. You must differentiate between peritonsillar cellulitis and retropharyngeal abscess. Your differential should include other don’t miss items such as epiglottitis, Lemierre’s syndrome, Ludwig’s angina, and angioedema.
UpToDate has a helpful algorithm on the diagnosis and treatment of peritonsillar abscess in the ED.
Management:
Antibiotics: Mandatory
PTAs are often polymicrobial. Antibiotics should cover group A strep, respiratory anaerobes, and staph aureus
First line: ampicillin/sulbactam 3 g every 6 hours
Alternatives: clindamycin +/- levofloxacin, metronidazole + penicillin G, or ceftriaxone
Add vancomycin (or linezolid) if MRSA suspected or severe infection
Obtaining culture is rarely (if ever) warranted
If patient is ultimately able to be discharged, can transition to PO amoxicillin/clavulanic acid vs clindamycin for 10-14 days total
Steroids: somewhat controversial
A systematic review by Hur et al., 2017 of three RCTS totaling 153 patients (unable to pool given heterogeneity) administered adjuvant steroids after PTA drainage, showed statistically significant improvement in body temperature in all three RCTs. Pain scores, mouth opening, time to painless oral intake, and hospitalization duration had statistically significant improvement in one or two of the three RCTs
I typically give a single dose of dexamethasone, especially if it’s a large PTA
Pain control:
NSAIDS are a great first line if no contraindication
Topical and local anesthetic
Imaging: CT vs US
A small, prospective study, (Scott et al., 1999), showed that physical exam alone is insufficiently sensitive (78%) or specific (50%) in distinguishing between PTA and peritonsillar cellulitis, as compared to CT (100% sensitive, 75% specific) and intraoral US (89% sensitive, 100% specific).
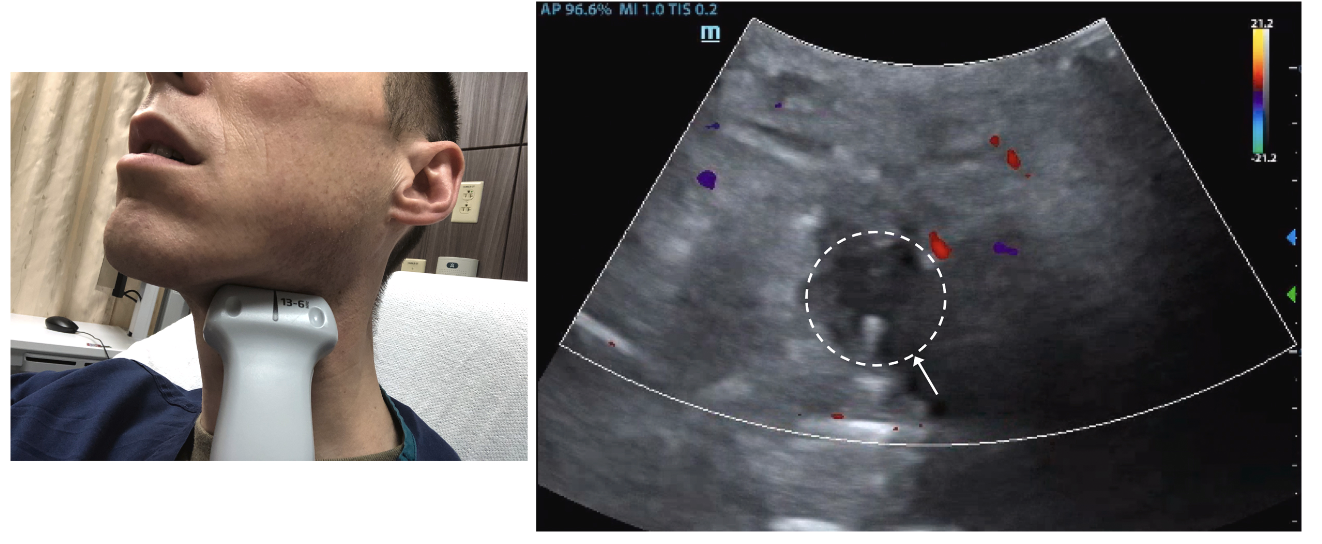
A systematic review and meta-analysis (Kim et al., 2023) of 17 studies with 812 patients (all cohort studies aside from one small RCT), intraoral US was 91% sensitive and 75% specific for PTA, while transcervical US was 80% sensitive and 81% specific.
If the endocavitary probe is available and its use is logistically feasible, this is my preference. Otherwise, my practice has been CT with IV contrast. Transcervical US is markedly less sensitive but it could be an option in certain settings.
Surgical drainage: needle aspiration vs incision and drainage
Needle aspiration has long been the preferred initial surgical drainage technique over scalpel incision and drainage
Chang et al., 2016 performed a Cochrane systematic review and meta-analysis of 11 studies (614 patients) that compared needle aspiration with incision and drainage. There was significant heterogeneity among studies and outcomes were not measured consistently. I+D was associated with lower PTA recurrence rate, but associated with more pain. There were only a few adverse events/complications total–all were I+D. Deemed existing evidence “very low quality”.
Medical management alone vs surgical drainage:
Forner et al., 2020 performed a systematic review and meta-analysis of medical intervention alone vs surgical drainage. It included 33,468 patients from largely observation studies: 10 cohort studies and two randomized studies. Of the two randomized studies, one was a small randomized prospective cohort study, and the other a very small RCT that was not peer reviewed and did not have a published manuscript. It showed no statistically significant difference in treatment failure of medical management alone (5.7%) vs surgical drainage (5.5%). And was a very heterogeneous group of studies with poor quality of evidence. There was also a clear treatment bias in that more severe abscesses are more likely to experience treatment failure and complications, and are more likely to be treated surgically. Whereas, less severe disease is more likely to be treated medically.
My take on this: I do not think there is sufficient evidence to routinely treat these with medical management only.
One of these retrospective cohort studies, Battaglia et al., 2018, compared a random sampling of patients from 12 Southern California Kaiser centers which adopted a PTA algorithm of medical management and ENT follow up the next day, with subsequent I+D if needed vs patients from seven centers in the same system that opted for initial surgical drainage. These were reviewed from the charts of patients 10 years prior. Treatment failure was defined as requiring a subsequent surgical drainage in the next 42 days. 8.1% in the medical cohort and 6.2% in I+D cohort met criteria for treatment failure.
In 2018 EMRAP reviewed this abstract, and although there was some nuance in their discussion, the editor’s commentary in the show notes states “This practice changing paper shows that you can decide to treat a PTA [with] steroids and antibiotics and expect similar results to an I+D procedure. The catch is that these patients must have improvement following initial therapy and scheduled follow up to assess the need for a delayed I+D”.
My take: This is quite a strong statement for a retrospective cohort study. More and better-quality evidence is needed before changing our practice.
But this and the systematic review of existing literature could potentially reassure us somewhat if we get a “dry tap” on needle aspiration, assuming appropriate return precautions.
Complications:
Incomplete drainage–also called “dry tap”
Recurrence
Post-procedure bleeding
Carotid artery injury
Particularly if an aberrant internal carotid artery or internal carotid artery aneurysm is misdiagnosed as a PTA
Further illustrates importance of imaging (especially POCUS with doppler) over physical exam alone
My practice to this point has been needle aspiration in conjunction with medical management–and after my review of the literature, it will continue to be so. I could envision escalating from needle aspiration to I+D if there were a large abscess on imaging and I got dry tap, however I would discuss with ENT prior to the I+D.
EMRAP has a helpful procedure video that I recommend. And here’s another EMRAP video with both needle aspiration and I+D
ALiEM, emDocs, and EMRA also have excellent blog posts on the procedure
Intraoral POCUS with endocavitary probe and PTA drainage with needle aspiration:
Medical management and pain control (as described above)
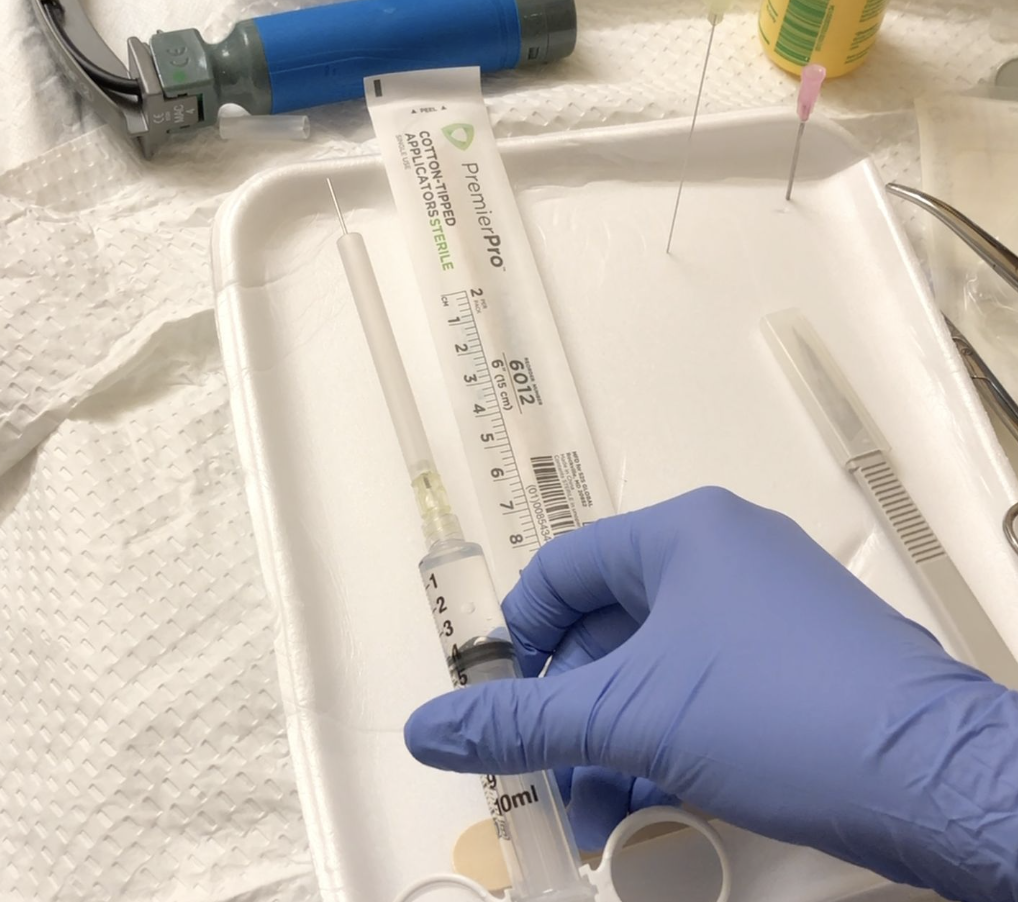
Gather your equipment
Ultrasound with disinfected endocavitary probe in sterile cover
Topical benzocaine spray (Hurricane Spray vs other topical)
1-2% Lidocaine with epinephrine and 25g needle and 10 cc syringe
Both for numbing and vasoconstrictive properties to minimize bleeding
Standard geometry laryngoscope
I’ve used both VL and DL (Macintosh 3 or 4) with success in the past
Yankauer attached to suction
Airway equipment prepped at bedside in the rare event of airway compromise secondary to severe hemorrhage or obstruction
18-20 gauge spinal needle with needle guard attached to 10 cc syringe
Scissors or sterilized trauma sheets
Place patient on monitor
Topical anesthetic
I recommend doing this prior to intraoral POCUS
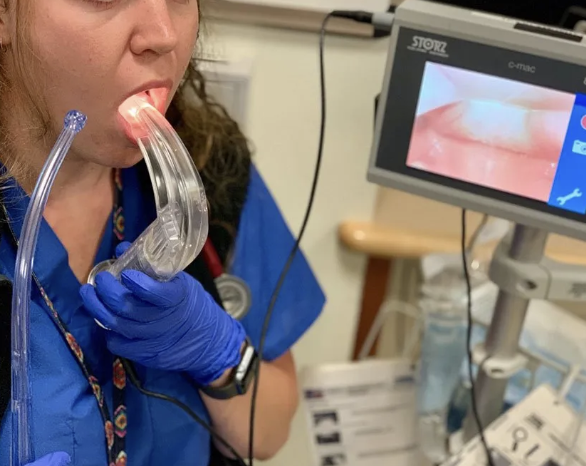
With patient sitting upright in bed (and head against headrest) have them hold the Yankauer in one hand and the laryngoscope in the other hand
Spray topical benzocaine (Hurricane spray) for about a half second over the PTA, allow patient to suction with the Yankauer after
There’s a small risk of methemoglobinemia, so don’t over do it with the Hurricane spray
Can alternatively nebulize 2-4% lidocaine without epinephrine over 5 mins
Insert endocavitary probe intraorally
Can ask patient to help direct probe to area of maximum tenderness
Fan superiorly and inferiorly (most PTAs occur in the superior pole)
Measure in two planes to estimate the volume and depth of the abscess from the surface
Also use this to visualize where the PTA is deepest and where you will most likely succeed in aspirating as much of the abscess as possible
Use color flow doppler to identify the carotid artery
This is for static ultrasound guidance, which is how I’ve always done it. Hennepin Ultrasound has a blog post on how to perform this both statically and dynamically–visualizing the needle as it aspirates the PTA.
Remove the sheath from your 18-20 gauge spinal needle and cut the distal portion of your sheath to a length that is a bit less than the deep wall of your abscess. (And well before the depth at which it would reach the carotid). Then place the cut sheath back on your spinal needle.
Inject about 5 cc of 1-2% lidocaine with epinephrine into the PTA
Having already identified the largest fluid pocket with US, insert your spinal needle (with cut sheath over it) into the PTA and aspirate
If patient is appropriately holding the laryngoscope and giving you a great view, with the tongue depressed adequately, you have both hands free and can use one hand to stabilize the syringe and the other to aspirate
Otherwise, if you have to hold the laryngoscope, do so with your non-dominant hand. Use your dominant hand to hold the syringe and withdraw and aspirate using the same one-handed technique that you do during a central line
May require multiple attempts or may have more to drain after first attempt
If unsuccessful, withdraw syringe and redirect the needle, aiming towards where the ultrasound identified the largest pocket
My most successful PTA aspirations were using POCUS with the endocavitary probe. However, if still unsuccessful consider getting additional static views with the endocavitary probe vs using dynamic guidance. Can additionally consider a landmark approach: attempting to aspirate the superior pole, and if still required can attempt drainage at the middle pole, and consider aspiration of inferior pole with caution.
Moving laterally and inferiorly increases the risk of carotid artery injury. However, having identified the depth of the abscess and the depth and location of the carotid artery, this decreases the risk of this complication.
Post Procedure:
Monitor and allow patient to continue to suction with the Yankauer
Have patient gargle water to promote continued drainage
After successful procedure, if post-procedure bleeding is minimal, and the patient’s clinical picture is otherwise reassuring, they can be discharged. Discharge with PO antibiotics (typically amoxicillin/clavulanic acid), strict return precautions for worsening bleeding, inability to tolerate PO, worsening infection, etc. Ensure discharge with close follow up.
If complications, persistent bleeding, persistent trismus, concern for airway obstruction, may require further surgical drainage by ENT vs admission (or observation) for IV antibiotics, medical management, and continued monitoring in conjunction with your consultants’ recommendations.
And there you have it! A lot of times we consult ENT and they perform the aspiration, but it is well within our scope of practice to do it ourselves! And POCUS with the endocavitary probe will help to maximize your success!
UpToDate has a helpful algorithm on the diagnosis and treatment of peritonsillar abscess in the ED.