So you’re in the ED and a G9P8 patient at 40w2d rolls in with contractions every 3 minutes. Before sending the patient upstairs you do a brief examination and you see this…

You deliver the baby flawlessly and even protect the perineum like a pro; however, the baby is quickly followed by the placenta and then a gush of blood that won’t quit.
Postpartum hemorrhage can be scary and for good reason. It is a significant cause of maternal mortality during childbirth, but is not something we often have to manage ourselves. It usually occurs after delivery of the placenta, but can occur at any time. Uterine atony is the most common cause and can be the entire uterus OR only the lower uterine segment, which may only be appreciated upon internal vaginal examination.
Besides complaining that OB hasn’t returned your page, these are 5 things you can do to help save your patient:
1) Pain control – This allows for proper examination technique and firm uterine pressure. Watch out for opioids that may lower blood pressure, especially morphine. Think fentanyl, just like in trauma.
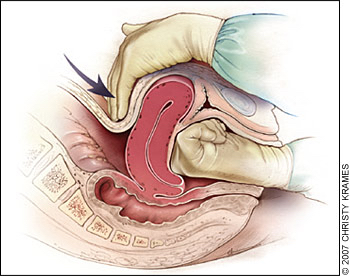
2) Uterine massage – In order to effectively compress the uterus, this must be done using a bimanual approach. Simple external fundal pressure may not be enough to stop the bleeding (see picture below). If you find retained products it may be helpful to remove them.
3) Oxytocin – Uterotonic agent that helps constrict bleeding vessels. No clear optimal infusion rate has been established, but more is not always better as rapid infusion can cause hypotension and CV collapse.
If no IV access, give 10 units IM. Once an IV is in place, you can inject 40 units of oxytocin into 1 L of normal saline and infuse 250cc/hr. Once bleeding is controlled, slow the infusion quickly.
4) TXA 1g IV – The World Maternal Antifibrinolytic Trial (WOMAN) was a randomized, double-blind, placebo-controlled trial that found administration of tranexamic acid was associated with a 19% relative reduction in maternal mortality.
5) Transfusion – Massive transfusion protocols aren’t just for trauma patients and GI bleeders! Active early, you can always send blood back if needed. Platelets, FFP, and pRBC ratios are not well established in postpartum hemorrhage, but remembering the concept of 1:1:1 ratios in trauma patients may be useful here as well.
Other measures such as balloon tamponade with a Blakemore tube or additional uterotonics will not be discussed here but are theoretical options.
TL;DR…
Page OB then:
1) Fentanyl
2) Bimanual uterine massage (internal and external, clear POC)
3) Oxytocin 10U IM, and/or 40U in 1L @ 250cc/hr (10U/hr) IV
4) TXA 1g IV
5) Massive Transfusion Protocol
Sources:
Crowning Baby Cake. Digital Image. Pelvic Health and Rehabilitation. 2018. https://pelvicpainrehab.com/female-pelvic-pain/4775/preparing-your-pelvic-floor-for-labor-and-delivery/
Bloody Mary Cocktail. Digital Image. Real Housemoms 2019. https://realhousemoms.com/bloody-mary-recipe/
Anderson JM, Etches D. Prevention and management of postpartum hemorrhage. Am Fam Physician. 2007 Mar 15;75(6):875-82.
Belfort, MA. Postpartum hemorrhage: Medical and minimally invasive management. In: UpToDate, Barss, VA (Ed), UpToDate, Waltham, MA, 2019
