As Emergency Physicians, the treatment of acute pain is our forte! However, it can become more challenging when patients with chronic pain—often on baseline prescribed opioids—present with severe or breakthrough pain. Likewise, converting between opioids or changing to IV formulations can be confusing and intimidating.
One of the easiest ways to get started is by calculating the patient’s total daily Oral Morphine Equivalents (OME).
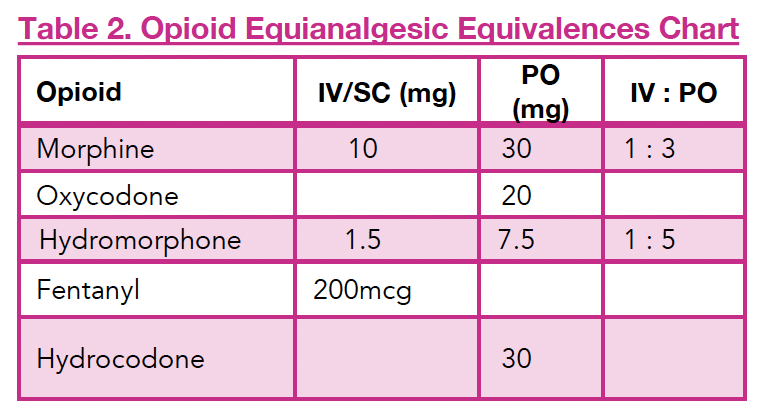
Example: Your patient takes 30 mg PO oxycodone TID and an additional 15 mg BID PRN for breakthrough pain.
- That totals approximately 120 mg of oral oxycodone in 24 hours.
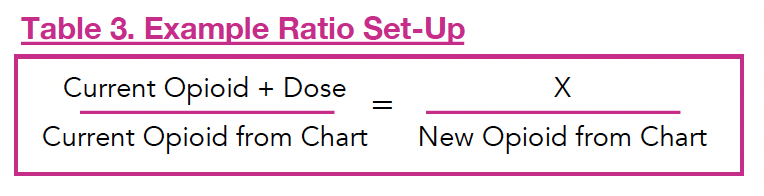
- Using Table 2 and 3, you can convert to 180 mg of oral morphine equivalents (OME).
- To convert to IV morphine: divide by 3 → 60 mg IV morphine/day.
Adjusting for Incomplete Cross-Tolerance
Before initiating a new opioid, consider reducing the dose to account for incomplete cross-tolerance:
- Well-controlled pain: reduce by 50%
- Moderately controlled pain: reduce by 25%
- Uncontrolled pain: no dose reduction
In this case, let’s assume the patient’s pain is not well controlled, so no adjustment is made.
Calculating a Starting Dose
Now that you know the patient is receiving the equivalent of 60 mg IV morphine/day, you can calculate a starting dose.
A safe place to start is to give 10% of the 24-hour dose as a PRN dose: 6 mg IV morphine.
Reassess and Titrate
Reassess pain 15 minutes after IV administration:
- Severe pain: give 100% of the cumulative dose (e.g., another 6 mg)
- Moderate pain: give 50% of that dose (e.g., 3 mg)
- Mild or tolerable pain: no further dose needed
Your goal is not zero pain, but a 50% reduction or mild, tolerable pain.
Establishing a Standing Dose
Let’s say your patient required an additional 6 mg IV morphine over the span of 4 hours. Their total dose for that period is now 12 mg IV morphine. This can now serve as the basis for a standing dose going forward.
Final Tips
- Be vigilant for sedation, respiratory depression, or other side effects, especially during titration.
- Morphine is a great first-line opioid. However, for patients with renal or hepatic impairment (e.g., GFR <30), consider:
- Using lower doses
- Extending dosing intervals
- Or switching to hydromorphone, which is safer in renal dysfunction. You can use the conversion table to calculate the appropriate dose!
