| Conference Summary: October 5th, 2022 Psychiatry Day |
| Complied by Lara Silverman MD/MPH, Emergency Medicine PGY3 |
| Alcohol Withdrawal with Dr. Olmedo |
| Intro: The lecture starts with a story about “Jack, who had been drinking for 78 days” and then suddenly stopped drinking. Within 12 hours of his last drink, he became weak, sweaty, nauseous, tremulous, and started having auditory hallucinations. Within 4 days, he saw animals coming out of floors and snakes spitting acid on his face. You might think this patient sounds like a perfect candidate for CPEP, until you look at Jack’s vitals, and realize he’s tachycardic, hypertensive, hyperthermic, and a little tachypnic. Jack’s brain wasn’t well, but it wasn’t because of a primary psychiatric disorder. Chronic alcohol use had changed his underlying brain chemistry and was now hyper-reactive. Also, alcohol causes lots of badness. 50% of MVAs and fires and 67% of homicides involve alcohol use. Some studies have shown that 25% of all patients BIBEMS to Emergency Departments have acute alcohol intoxication. Pathophysiology of alcohol withdrawal: In short, alcohol is a CNS depressant. It acts on GABA receptors to enhance inhibitory messages and slows the brain down. It also has inhibitory effects on the excitatory NMDA receptor. This also contributes to the overall depressant effect of alcohol. As long as you keep drinking, your brain will stay “in balance,” but within 12 hours of taking that alcohol away, your brain starts to become overactive and within 4 days, it’s completely unbalanced. It is worth noting that people who drink chronically can start to withdrawal even with blood alcohol levels in the hundreds. Syndromes involved in the presentation of alcohol withdrawal: The early stages of withdrawal can involve seizures (“rum fits”), hallucinations, and the classic “withdrawal” symptoms (tachycardia, HTN, hyperthermia, tremors, diaphoresis). These presentations can all lead directly to DTs, and the pathway is not linear.  Treatment of alcohol withdrawal: We used to treat these patients with restraints and antipsychotics, but obviously we now know that these symptoms are from alcohol withdrawal, leading us to use targeted therapies. Benzodiazepines and barbiturates are the mainstays and can work together to have a synergistic effect. They act on the GABA receptor, just like alcohol, so are great first line options. There are a few different approaches for initial management with benzodiazepines. You could front-load your patient and give a long-acting agent early. Alternatively, you could use a symptoms-triggered approach, which involves frequent reassessment. These two therapy options are associated with less overall medication required and shorter hospital stays. A frequent strategy employed, especially upstairs, is fixed-schedule therapy. This is convenient and protocoled, but results in more overall medication use and longer stays. Note that a lot of our frequently used benzodiazepines like midazolam (versed) are quick-on, but have been almost completely eliminated by the kidneys after about 6 hours. Consider something long-acting with active metabolites like a barbiturate or a long-acting benzo if you are worried about not staying on top of reassessment. The shorter acting agents will initially work just as well, but risk leaving the patient unmedicated. Careful not to fall into the trap of treating vitals. Patients are often tachycardic and hypertensive, but the underlying cause is a hyper-adrneergic state. Throwing medications like beta-blockers and clonidine at a patient with abnormal vitals from withdrawal will not address the underlying cause, CNS over-excitation. Adjuncts: Benzos and barbiturates don’t have a 100% cross-tolerance with alcohol, so occasionally, we will have to add additional agents. For this, we can consider propofol, which has NMDA activity, and precedex. Ketamine, an NMDA antagonist, can also be considered. Some anti-dementia NMDA antagonists are also currently being researched as adjunctive treatments. A note on aggressive treatment: The concept of kindling is important. Over time, seizures that occurred even from weak chemical or electrical stimuli cause “scarring” in the brain. This scaring predisposes the brain to having seizures in the future. This theory supports the aggressive treatment of even mild withdrawal. Keeping a pt from having a first seizure can stave off the kindling process. If a patient has a history of withdrawal seizure, we worry about this patient seizing earlier than we might otherwise expect. Over time, this also contributes to alcohol-related brain damage and cognitive impairment. Treatment of alcohol withdrawal seizures: Organic seizures excluded, phenytoin and placebo are equally good at treating alcohol withdrawal seizures. So if your patient has no underlying seizure disorder and you suspect alcohol withdrawal seizure, go straight for your benzos. Also important to note, many of the medications we use for agitation (haldol, phenothiazines, butyrophenones, etc.) lower the seizure threshold. These can be used very effectively to treat agitation, but use with caution. When do patients die from withdrawal?: The mortality of Delirium Tremens used to be around 20%. However in this day and age, we have lots of tools in our toolbox to treat withdrawal. With supportive measures, critical care, electrolyte and vitamin repletion, and targeted medical sedation, isolated withdrawal is a condition that should have a mortality of 0%. However, there are many concurrent pathologies that still lead to mortality. For example, 75% of patients with withdrawal seizures had a temperature greater than 103.9! Put this patient in an ice bath, cool their brain, and keep their proteins from getting disnatured. Also, patients in withdrawal have stopped or slowed drinking. But why? Was it due to underlying infection? Trauma? A heart attack? Always be thinking about what else is going on. Pitfalls: Don’t assume anything in these patients, we’ll miss big stuff. Some of our common pitfalls: Assuming AMS is a result from only alcohol withdrawal (these patients also have high incidence of infection and trauma)Treating vitals, not clinical pictures Treating severe withdrawal with oral and IM meds (these have erratic or delayed absorption)Over-sedating patients and causing respiratory depressionAssuming bad vitals are just from withdrawal (not from that giant aortic dissection we’re missing) |
| Small groups |
| The Agitated Patient (Drs. George, Goodin, and Walther): This focused on the initial assessment and management of an agitated patient. Walk into a room, first assess for scene safety. Make sure you and your team have good PPE and there are enough people to restrain a patient. Ideally, you will have 5 people: one for each limb and one to watch the patient’s airway. Try to place the patient in 4-point restraints if possible and use IM sedation (because usually we don’t have an IV and this is safer, needle-stick wise). Always try to remove restraints as soon as possible. Interestingly, if a patient speaks ALS, it is recommended that restraints be removed ~once per hour to allow them the opportunity to communicate (if restraints are still needed at all). For sedation, our mainstays are benzos (ativan/lorazepam — slower on, longer lasting, midazolam/versed — faster on, shorter lasting) and the antipsychotics (haloperidol and droperidol). Beware that benzos can cause respiratory depression and antipsychotics can cause QTc prolongation. Always get an initial EKG and put the patient on a monitor. An alternative medication to consider is IM ketamine. Note that the IM dose of ketamine is high (400-500) and very different from the IV dose. Also, some institutions give cogentin and/or benadryl prophylactically. In general, try to save these only for the patients who exhibit pyramidal symptoms. Finally, what about your psych patient who is refusing blood draws? Are they allowed to? Short answer: yes, if they have capacity (see Decision Making Capacity with Dr. Schwartz below) and you’ve ruled out life-threatening issues / underlying medical causes for their presentation. Imaging Review with Dr. Geoff: Go here: https://www.casestacks.com. Awesome stuff. Suicide Assessment with Dr. Schwartz: Dr. Schwartz is double-board-certified in EM and psych. Cool! He talked to us about suicide assessment. The big take home points here are to consider the whole clinical picture and if you have any doubts at all, talk to family members. A thorough assessment of suicidal ideation isn’t just about the moment we see a patient in the emergency department, when they might be intoxicated or agitated. These patients should have: 1) a good history taken as well as a good chart check. Really try to understand prior psychiatric history, prior self harm behavior, or prior suicide attempts. 2) a physical exam to assess for recent or prior engagement in self harm 3) involvement or input from a family member (SO important!) |
| Medical decision making capacity with Dr. Schwartz |
| When assessing capacity, you must always weigh the consequence of a patient not receiving medical care versus a patient being stripped of their capacity, which can affect their trust of the medical system, their dignity, and their autonomy. We have a huge responsibility to make this decision correctly. What is decision making capacity?: The patient should understand their medical conditions, the various decision pathways, and the consequences of each. They should ideally not only be able to answer “yes” when asked “do you understand,” but should be able to demonstrate to you in plain english (or their native language) the ability to reason through their current circumstance and the potential consequences of various options. Pay special attention to consistency in values. It doesn’t matter if you disagree with a patient’s logic, it just matters that the patient’s logic is consistent with the patient’s own belief system. To emphasize this, Dr. Schwartz told a story about a patient who deeply distrusted the medical system. When he presented with a fall on eliquis and potentially life-threatening injuries, he refused treatment, as his experience with the healthcare system led him to believe staying in the hospital was likely to cause him more harm than good. Whether or not we agree with this, the patient’s desire to not be treated in the hospital was consistent with his personal belief system, which he was able to vocalize. This consistency between values and medical decisions is important when determining capacity. Intoxication: Intoxication is a complicating factor. The degree to which intoxication is either preventing logical reasoning or altering a patient’s values should be considered. Intoxication can, but doesn’t necessarily have to, prevent someone from having capacity. This determination of no capacity can be reassessed and restored in times of sobriety. Framing the conversation: Finally, how we frame a conversation and approach a patient is important. In the early 60s, emergency medicine wasn’t yet a speciality. Physicians often had life-long relationships with their patients. Now, we meet patients for the first time often in situations of high stress, but it takes time to adequately understand a patient’s situation. In the most challenging cases, we can turn to our psychiatric colleagues. However, Dr. Schwartz had some helpful advice on how to frame the conversation and approach the patient. Don’t try to “convince” a patient of anything. Be open-minded and have the patient explain what will be most beneficial for them. In some cases, this will be leaving against medical advice. Dr. Schawartz also recommends being informal and emphasizes trying to be an ally for the patient. Get to their level physically (lean over, take a seat) and help them feel like you’re not in a rush and that they, their health, and their wellbeing is important to you. Don’t use medical jargon, speak in simple terms, and, if you can, involve the family even if just over the phone. Hopefully, by the end of a genuine conversation, you will have determined if a patient has capacity: they understand their medical situation and the consequences of various options, and their logic is in line with their belief system. |
| Case Review Series with Dr. De La Cruz |
| Know the types of Myocardial Infarctions! Types I MI: From plaque rupture leading to thrombus, compromising blood flow Type II MI: From (almost) everything else (“demand ischemia:” supply / demand issue exists due to atherosclerosis, decreased volume, vasospasm, coronary artery dissection, etc) 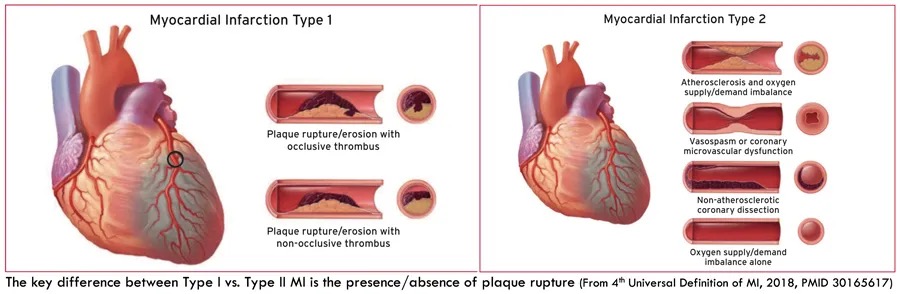   |
Get Dragon (dictation) on your iphone!! Everyone has access, but signing up is time sensitive!! Elmhurst as a hospital has finite spots, and they’re filling up!!Follow these steps, fill out the form, and that’s all there is to it!Go here. (https://nychh.service-now.com/sp?id=sc_cat_item&sys_id=8c0ec073db782300baec561bdc9619c0) 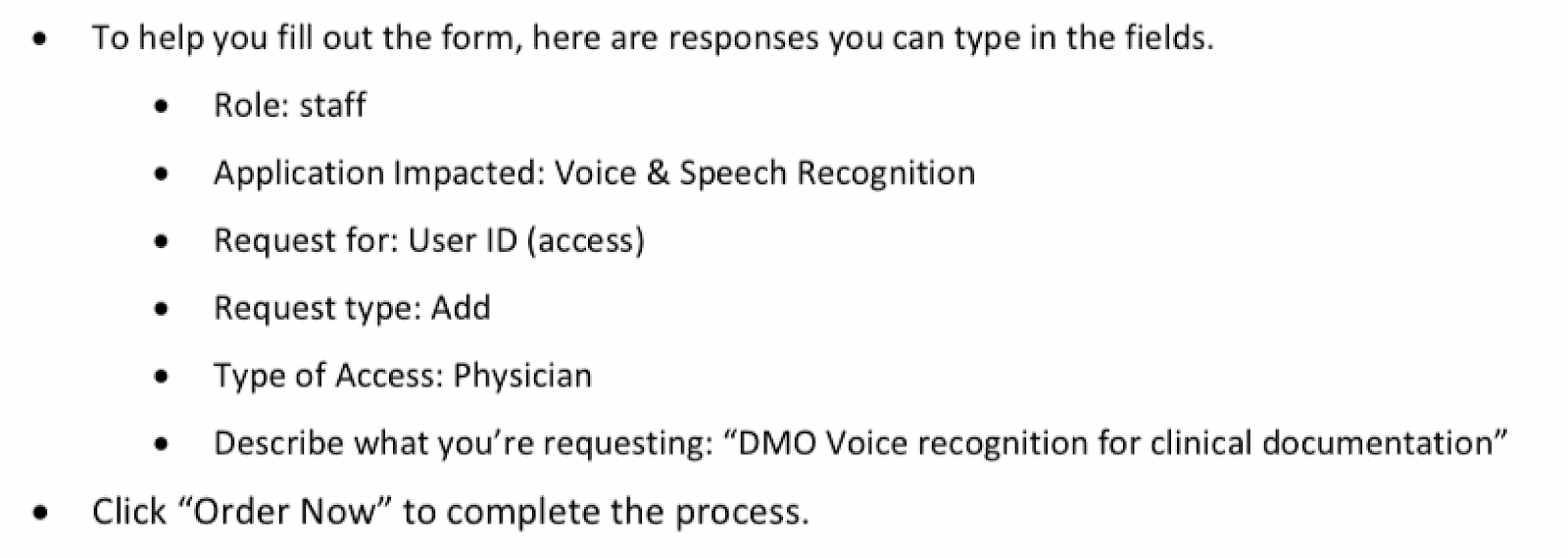 |
