If you were on a tea & toast diet, how much water would you need to drink before you develop hyponatremia? I haven’t seen anyone work out the numbers before so here are my calculations.
And the key to understanding hyponatremia is the renal handling of water.
Take-home points #1:
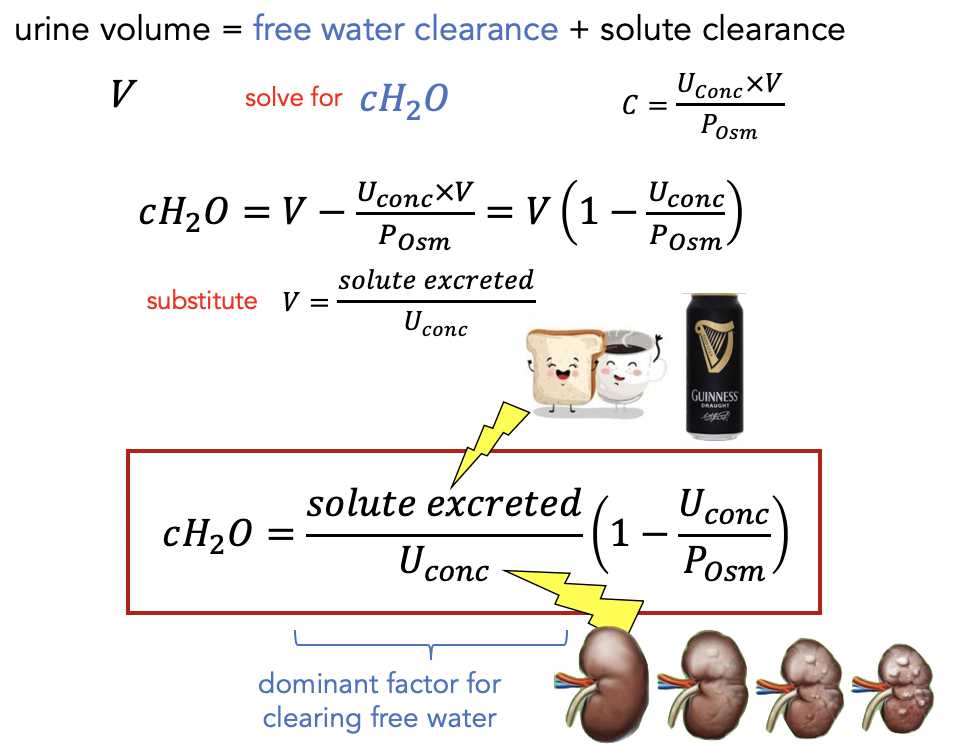
- water follows solutes ⟶ need solutes to excrete water
- the most dilute concentration of urine possible (assuming normal kidneys) ~ 50 mmol/L
- concentration = moles of solute / volume
Now consider eating only 5 pieces of toast and 2 cups of tea today. The only solutes that contribute to osmolar concentration arise from sodium (i.e. Na+ and Cl-, needs a ×2 factor) and protein: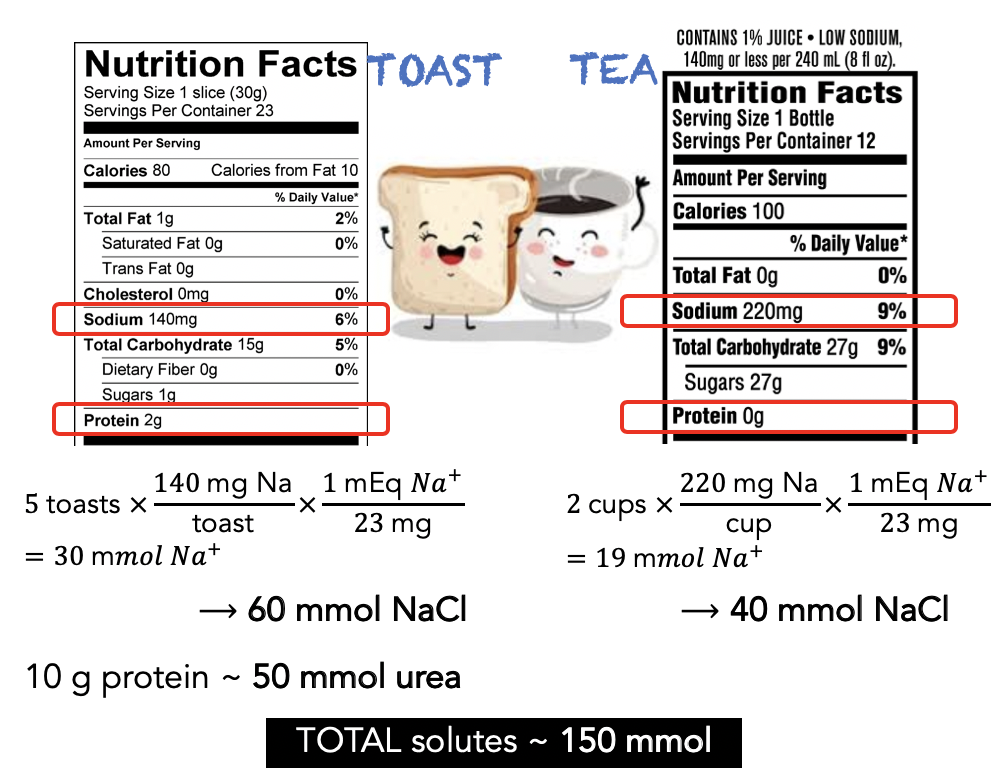
Note: the daily solute load is normally = 10 × weight (kg)
By substituting the minimum concentration and total solutes of a 2 tea & 5 toast diet and solving,
50 mmol/L = (150 mmol) / volume
Volume = 3 Liters
In other words, you will develop hyponatremia if you drink in excess of 3 L of water on this low-solute diet.
To review the example above, solutes are needed to excrete the water and the kidneys can only do so much to dilute the urine. Any more water above the minimum dilution will overwhelm the kidney and remain in plasma!
Take-home points #2: see hyponatremia…
- think: possible hypo-osmolality (key to pathophysiology behind neurologic sequelae)
- ask: why is there relative excess of water? (key to understanding the etiology)
Instead of memorizing hyponatremia flowcharts / algorithms, ask: “why is there an excess of water?” (sodium is paradoxically NOT the problem!)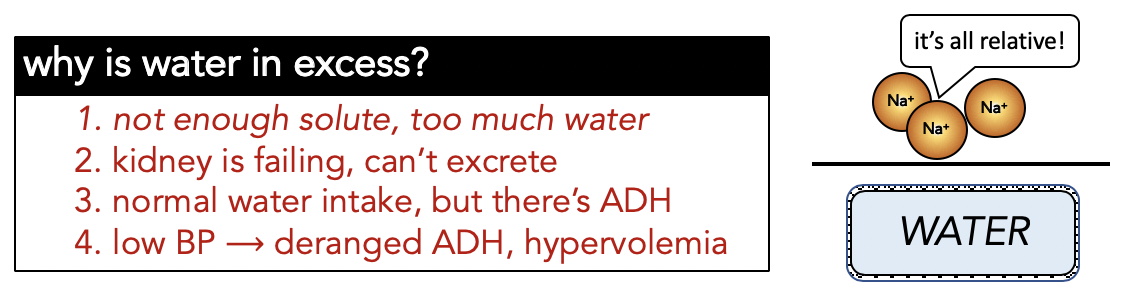
We know that in HFrEF the problem is pump failure, and even though the intravascular plasma volume is high, the BP (= CO x SVR) is sensed as low, leading to sympathetic response and R-A-A-S activation and ↑plasma volume (i.e.↑WATER). The issue with cirrhosis is ↓ systemic vascular resistance (SVR) leading to low sensed BP coupled with ↓oncotic pressure.
Etiology #3 will be covered in a future post, along with drugs and conditions associated with acute (< 48 hour) hyponatremia.
I’ve lost count the number of times I studied hyponatremia — it’s almost always confusing. I hope to fully understand the pathophysiology before I finish residency. Here are some of the best resources I’ve come across: EMcases, Curbsiders, PreciousBodilyFluids
Miscellaneous calculations (not crucial, but explicitly shows how water can be in excess):