Is it safe to give LR or plasmalyte to a hyperkalemic patient (these balanced crystalloids have 4-5 mEq/L K as opposed to 0 mEq/L K in normal saline)? Postponing the discussion of renal handling of potassium to review the physiology of fluid resuscitation in the setting of hyper K (per request by Dr Hickey). This has been debunked many times elsewhere, but here is my perspective as a chemist.
Fluids are medications, and we can do harm by ignoring the tonicity. Balanced crystalloids distribute into the extracellular space because they are nearly isotonic to plasma:
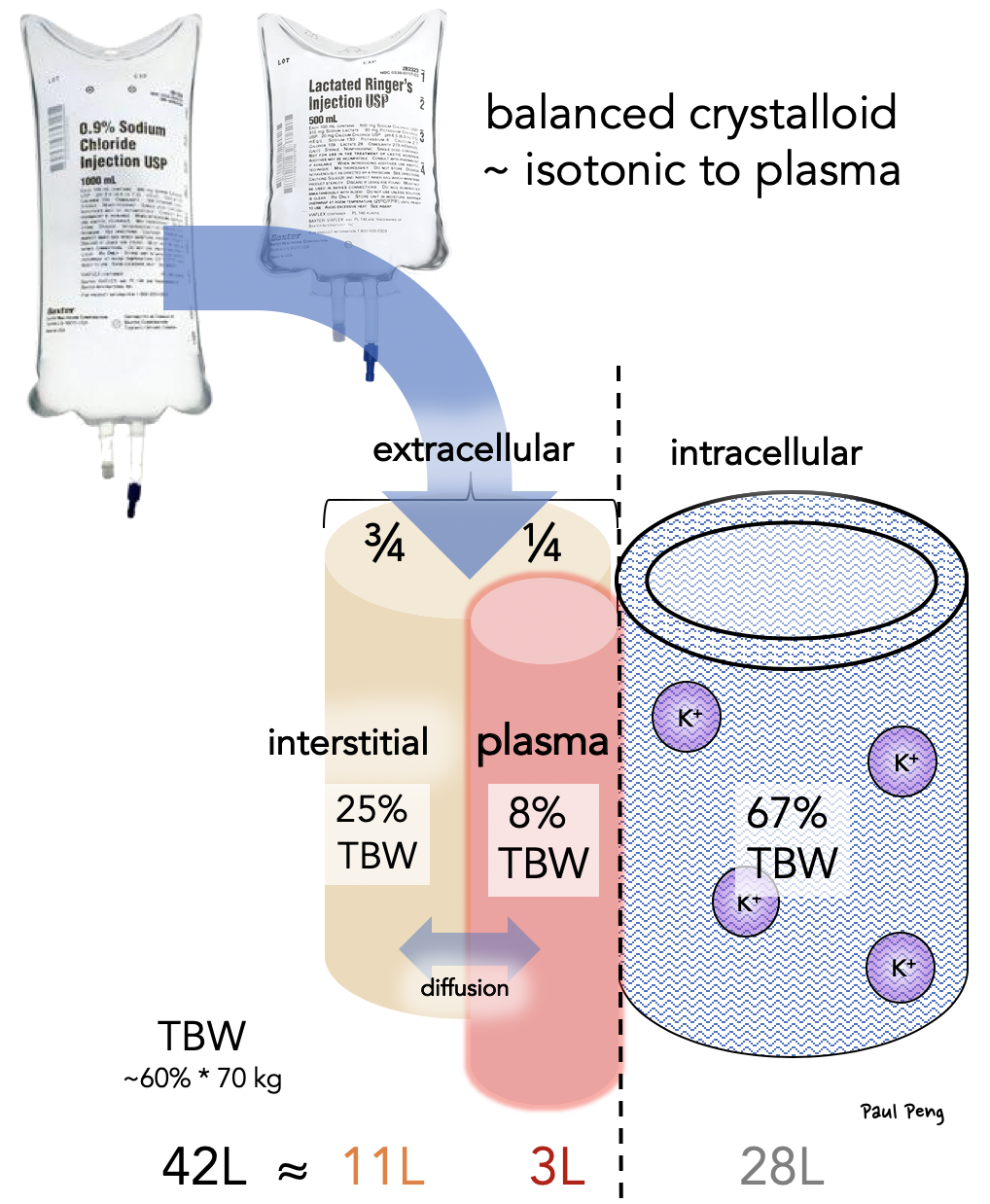
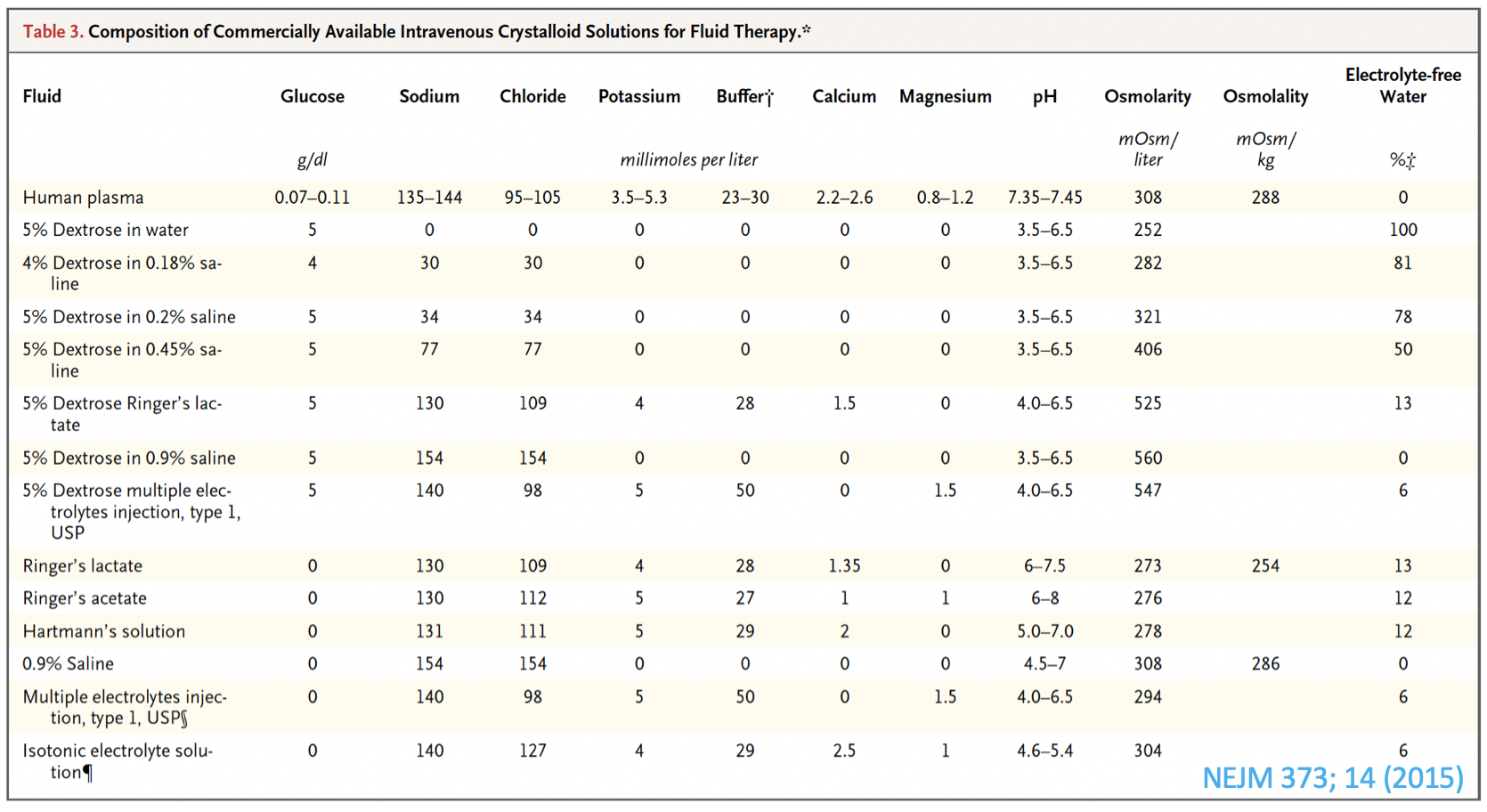
For resuscitation, we care about how much goes into plasma, which is only ~25%! So only 250 mL of a 1 L balanced crystalloid actually contributes to the intravascular space. Review why D5 (5% Dextrose) in water is not a resuscitative fluid. Here is a good table summarizing the compositions of fluids:
We should NOT be worried about LR or plasmalyte increasing the [K+] in a hyperkalemic patient who requires fluid resuscitation.
This is why:
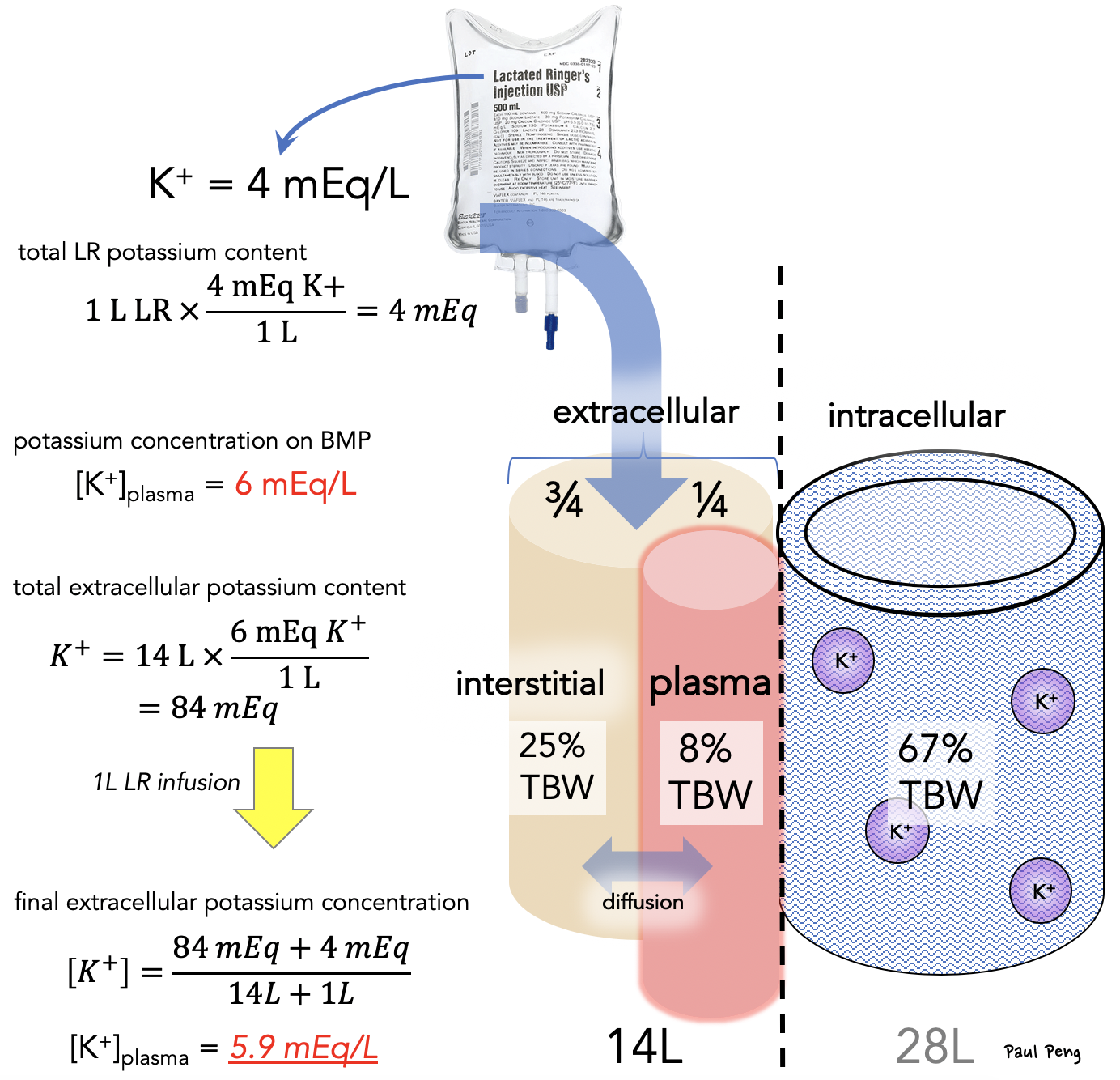
Basically, the contribution of the K from LR (i.e. 4 mEq total) to the extracellular space is relatively small. When the final K content is divided by the total extracellular volume, the [K+] actually decreases!
Check out actual data (Panel D) from the SALT-ED trial:
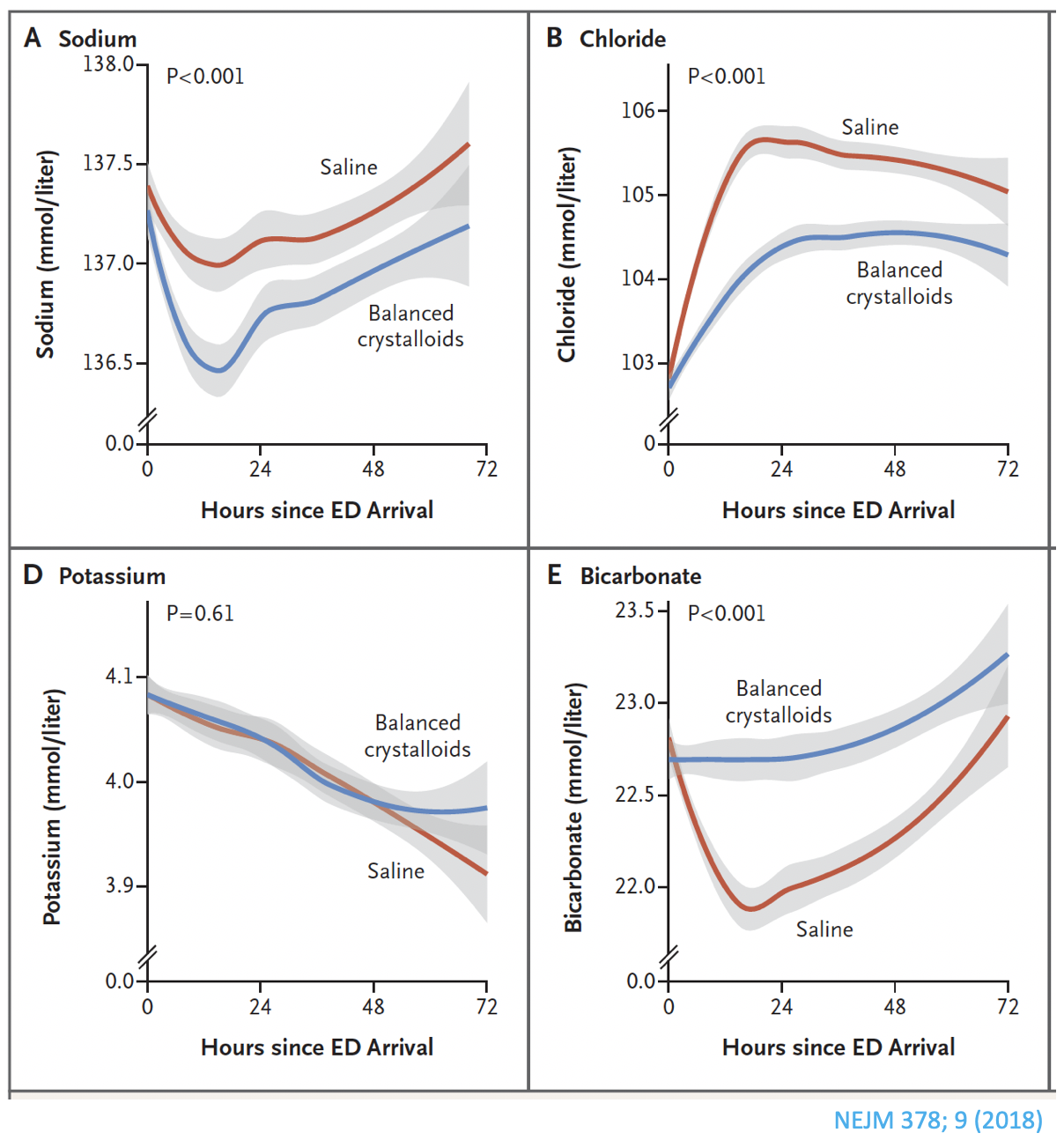 Even more interesting is Panel E… Why does the bicarbonate decrease with administration of saline? May have to postpone renal handling of potassium once again to review hyperchloremic acidosis, strong ion difference, and a new look at anion gap.
Even more interesting is Panel E… Why does the bicarbonate decrease with administration of saline? May have to postpone renal handling of potassium once again to review hyperchloremic acidosis, strong ion difference, and a new look at anion gap.
