You’re in the resus room having your morning bottle of water when the triage nurse rolls in your new patient. Diaphoretic, talking but lethargic appearing, and, when placed on the monitor, showing this:
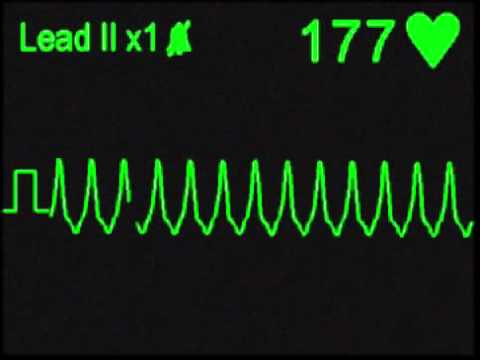
Being the astute resident that you are, you know this is VT and the next step is cardioversion in an unstable patient with this rhythm. You do the cardioversion and the rhythm improves. You walk away feeling good about yourself and while you’re putting in orders for your new patient your resus nurse calls you back to the bedside. You see your patient who was just speaking a little lethargic again and this:
You again cardiovert the patient, successfully, but you know now (because you’re astute, remember?) your patient might be in electrical storm and could deteriorate again. So what do you do?
Electrical storm, or incessant VT/VF, can be defined as 2 episodes of VT or VF within 5 min or 3 episodes within a 24 hr period. Incidence of this is low, but management can be difficult and morbidity can be high. So how do you save your patient? The step by step approach recommended is a combination of medications and cardioversion outlined below:
- ABCs first
- Unstable patients receive cardioversion/defibrillation as per ACLS
- Stable patients – amiodarone (150 loading +/- drip) is current recommendation though procainamide has shown promise in refractory cases
- Esmolol – part of pathophysiology appears to be sympathetic overdrive and a beta blocker will help with that
- Correct electrolyte abnormalities or other underlying causes if any found.
- Double sequential defibrillation – if defib indicated and the patient has been refractory can attempt this method. It basically increases power and has been shown to help with refractory cases.
- Catheter Ablation – most patients eventually need this so getting EP on board early is a must.
Bottom Line: Know the above algorithm so you know what the next step is for refractory cases and get cardiology involved early to help facilitate more definitive treatment (i.e ablation).
References:
- Passman, Rod. “Electrical Storm and Incessant Ventricular Tachycardia.” UpToDate, S.n., www.uptodate.com/contents/electrical-storm-and-incessant-ventricular-tachycardia#H5924542
- Zipes DP, Camm AJ, Borggrefe M, et al. ACC/AHA/ESC 2006 Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: a report of the American College of Cardiology/American Heart Association Task Force and the European Society of Cardiology Committee for Practice Guidelines (writing committee to develop Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death): developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Circulation 2006; 114:e385.
- Gorenek B, Blomström Lundqvist C, Brugada Terradellas J, et al. Cardiac arrhythmias in acute coronary syndromes: position paper from the joint EHRA, ACCA, and EAPCI task force. Europace 2014; 16:1655.
