[TR PEARL #4] Tap that? CSF Shunts
- CSF shunts – these are the most common pediatric neurosurgery procedure done in the United States.
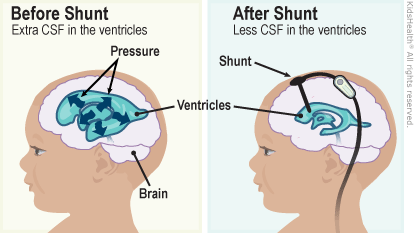
- A CSF shunt is placed in the ventricle to drain excess CSF when there is an obstruction in the normal outflow or when there is a decreased absorption of the fluid. Causes can include obstructive hydrocephalus (ventricular systems is blocked, and the CSF accumulates from a mass, tumor, cyst, aqueduct stenosis) to communicating hydrocephalus (subarachnoid system is blocked, and CSF can’t be absorbed – less common, but can be from from IVH, aneurysmal SAH, meningitis, post infection, post trauma, etc)
- While very common, these also have the highest rate of neurosurgical complications. About 50% fail within the first year, and the median survival of a shunt is usually 8-10 years, so a patient can expect 2-3 shunt revisions over the course of 20 years.
- There are three key parts to CSF shunts: proximal catheter (“ventricular catheter”), the valve, and the distal catheter.
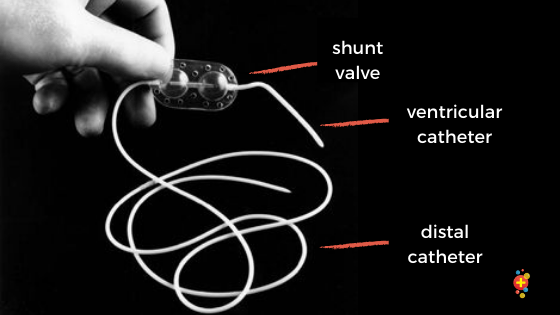
- The proximal catheter (“ventricular catheter”): Is placed through a Burr hole into the cerebral ventricle (often the R lateral ventricle to not disturb the dominant hemisphere).
- Shunt valve – the tubing is channeled through a “shunt valve.” When the pressure inside the brain is too high , the valve opens, allowing the CSF to drain. There are many different types of CSF shunts, and while they perform the same function, the key difference is the type of valves used and whether the valve is programmable or not to allow the team to decide when the CSF should drain. The entire structure is often called the chamber or reservoir.
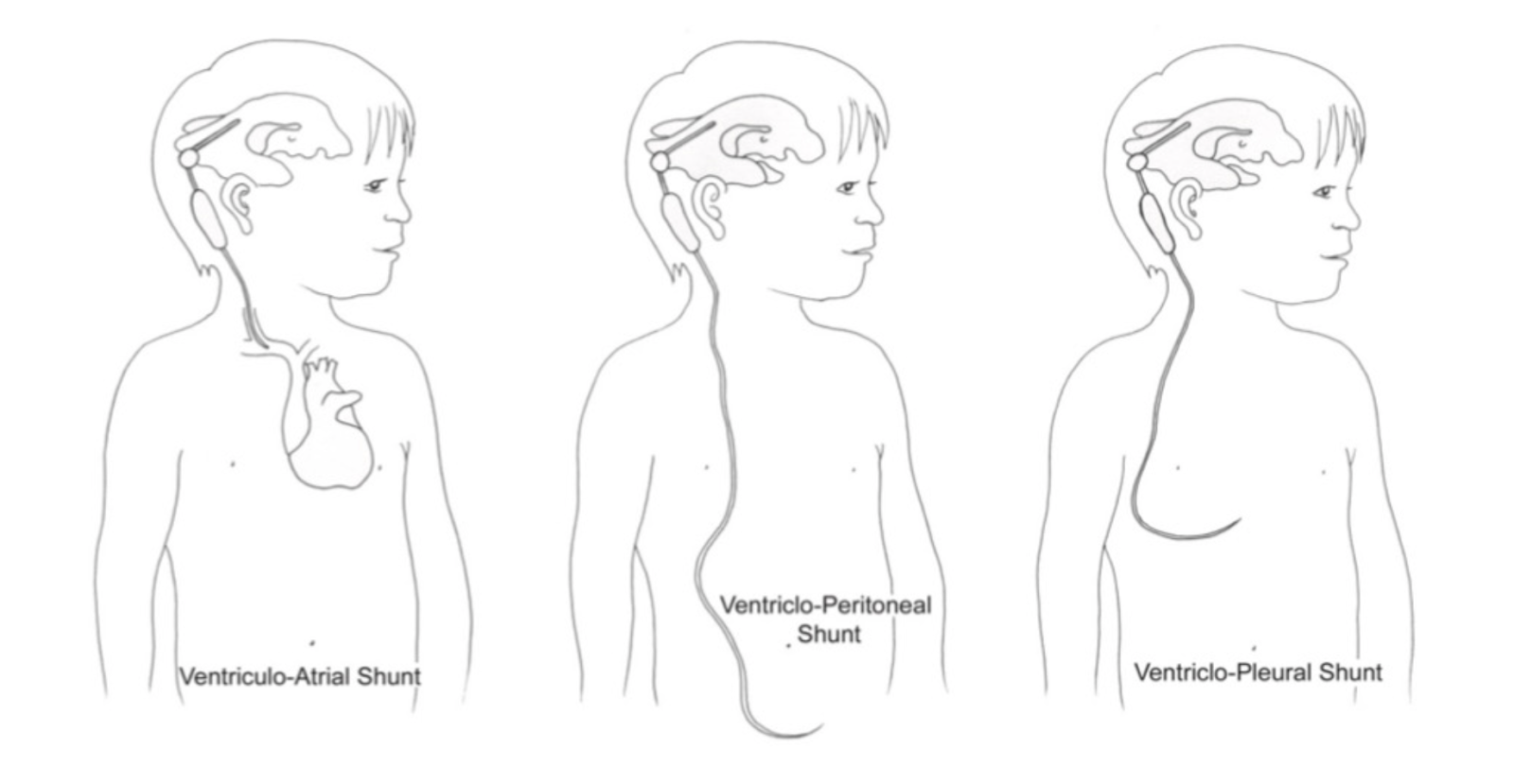
- Distal catheter: Drains the CSF either to somewhere inside the body or outside of it. Most commonly, they drain to the peritoneum – this is the classic ventriculoperitoneal shunt (VP shunt), but you can also see ventriculopleural shunt to the lungs (VPL), and ventriculoatrial (VA) shunt to the atrium even ventriculo-ureteric shunt (to bladder). Our trauma patients get CSF drain that drains to the outside world…the external ventricular drain, or EVD.
Types of shunt complications:
- Infection (5-15%)
- You can see signs of increased ICP such as headache, lethargy, AMS n/v, visual disturbances, or signs of infection such as pain/redness/tenderness around the tract. However, remember that fever is sometimes there, sometimes meningeal signs but they’re not always prent.
- The most common cause or complication of VP shunt infection is obstruction, mostly from skin flora.
- Note: Depending on the type of shunt, you may have different compilations. VP shunt infections can present with GI symptoms, peritonitis, as well as pseudocyst formation (localized abdominal fluid collections) around the peritoneal catheter, which will be asymptomatic until enlarged substantially to cause abdominal pain. VA shunts can present with endocarditis
- Dx: Infection confirmed with CSF fluid analysis and cultures. CSF is better obtained via shunt tap vs an isolated LP (see below). Consider abdominal U/s if the patient has GI sxs and you’re concerned for peritonitis/pseudo abscess.
- Txt: Empiric vancomycin (covers GPC) + cefepime (GNR) (+/- rifampin for penetration into CNS) => device removal and EVD once CSF is sterile. The treatment of shunt infections involves week to month-long admissions in the hospital.



- Shunt malfunction
- These are non specific, but you can see possible signs of increased ICP, as well as AMS (some estimate 100% PPV), headache, n/v/abdominal pain, lethargy, autonomic instability, and visual changes as well. Consider especially in patients with complex medical comorbidities, prior shunt failure, young patients/neonates.
| Obstruction (Underdrainage) – The most common etiology of VP shunt obstruction is infection! – You’ll see signs and symptoms of increased ICP – CT is likely to show increase in size of the ventricles and LP is likely to show an elevated opening pressure, not always | Overdrainage syndromes – Rapid drainage of CSF, when intraventricular pressure is less than the ventricular valve pressure – Intracranial hypotension: Cyclical, waxing and waning of presenting complaint, postural in nature, worsened when standing, relieved when lying down as ICP increases, the occluding tissue disengages, and, allows CSF drainage to continue. “Slit ventricles”: small ventricles predispose to catheter obstruction, with intermittent high pressure that allows the catheter to work again, only to have complete collapse to of the ventricles (SVS) again – Remember: SDH may occur due to tearing of bridging veins on brain collapse from overshunting | Malpositioning/Dislodgement – Can see localized pain, erythema, fluid at site, discomfort – This is one of the primary reasons why we get a shunt series. – May see signs of obstruction/increased ICP – But note, this does not always equate to shunt malfunction, as they might still continue to function through fibrous tract 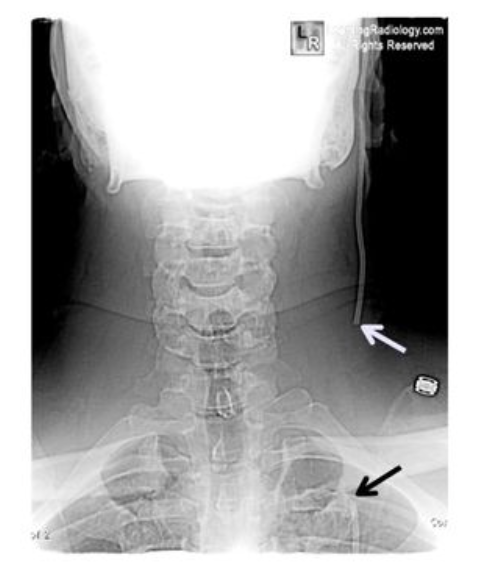 |
Workup and Management
How to examine the shunt?
In addition to calling neurosurgery and taking precautions if you’re worried about increased ICP…
- H&P – Identify the type of shunt & why they had to get the shunt. Have they had any revisions? Any failures?
- Some of the most common congenital causes include: spina bifida, hydrocephalus, Chiari malformations, dandy walker syndrome
- Acquired causes: tumors, IVH, infectious, arachnoid cyst, trauma
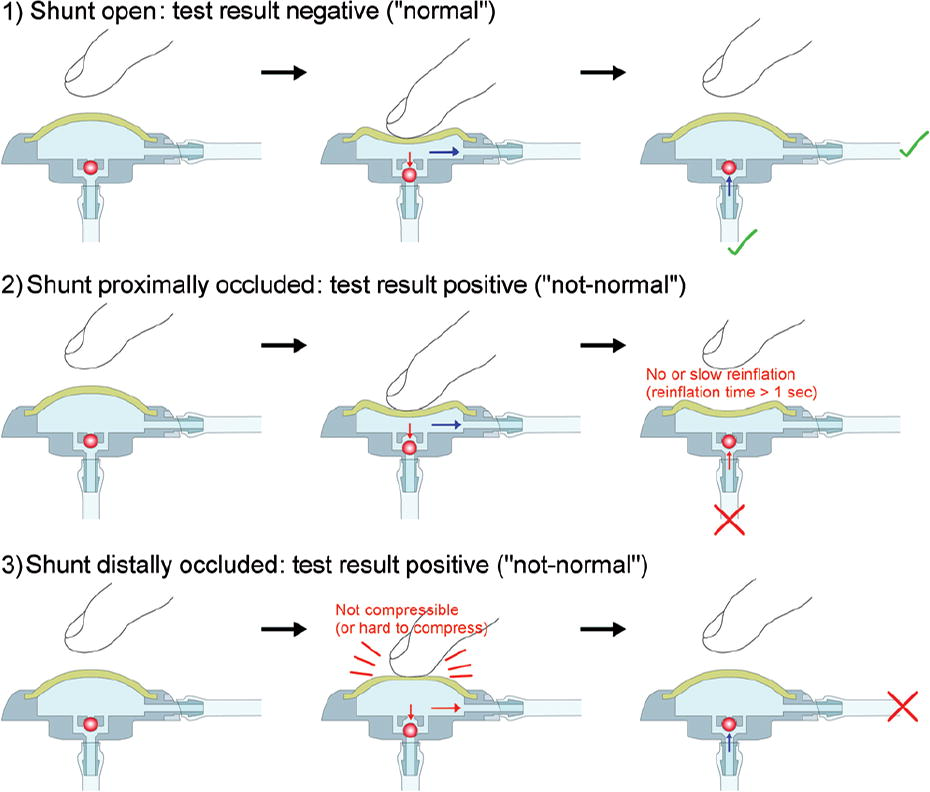
- Find the valve chamber (sometimes called the reservoir) & gently compress the chamber
- Difficulty compressing the chamber indicates distal flow obstruction
- Slow refill refill >3 seconds indicates a proximal obstruction
- This has sensitivity ~19%, specificity 80% of identifying shunt malfunction
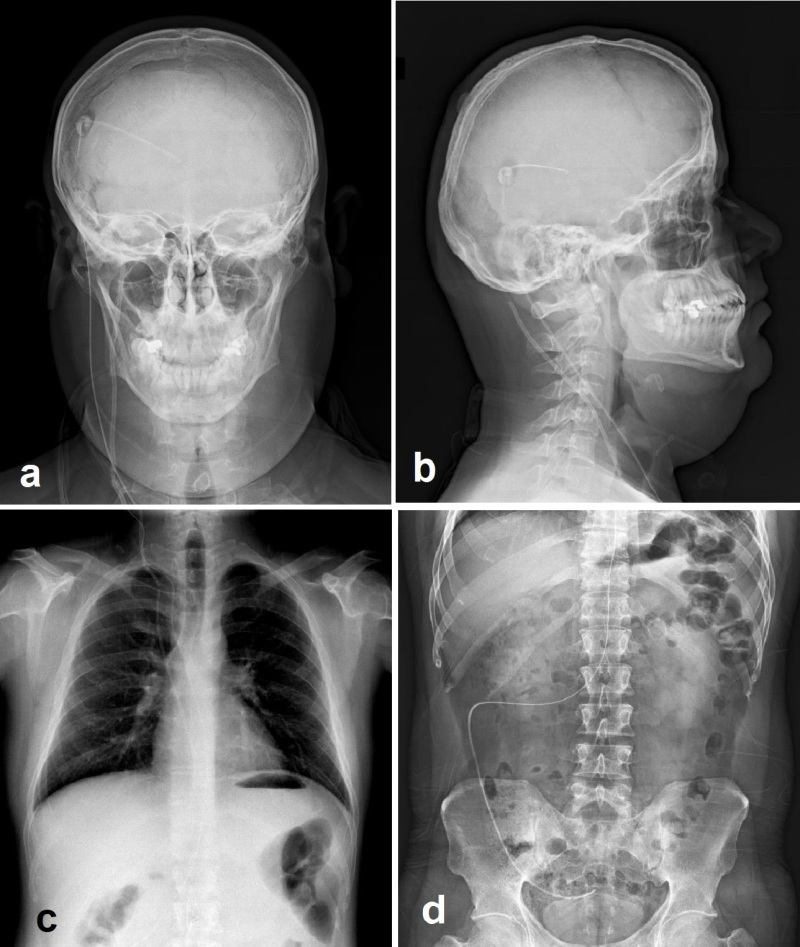
- Shunt series – plan radiographs to identify kinking, migration or disconnection of shunts system
- AP and lateral radiographs of skull
- AP view of chest and abdomen for VP shunts
- Head CT to eval for ventricle size
- You will need to compare to previous CT scans since many people will just have weirdly abnormal sizes
- But note, this doesn’t r/o shunt malfunction – Head CT only has a sensitivity of 83% for shunt obstruction, and 24% of patients with shunt malfunction did not show any radiologic evidence, ESPECIALLY in pediatric patients
- Note: these are MRI compatible, but the settings should be verified after exposure as the magnetic field can change programmable valves. The shunt should be checked by NSGY after
- Shunt tap – unless life saving, defer to our Neurosurgery colleagues to avoid damage to CSF valves. This being said, if there are life-threatening signs of impending herniation, and you need to transport patients and gain time before NSGY can take over, consider doing the tap. It is within the ED provider’s scope of practice.
- The indications of the Shunt tap: Diagnose infection, and also alleviate life threatening pressure. Can also give medications directly to the CSF, and evaluate the shunt function.
- Contraindication: Infection over the site of entry, bleeding disorder due to coagulopathy, lack of information such as the design of the shunt and the location of the reservoir
- Steps below:

| Gather the materials: – Sterile gloves – Sterile towels/gown – Antiseptic – betadine or chlorohexidine – Butterfly needle 23-25g – 3 way stop cock – LP kit – will need the CSF tubes, as well as manometry – Razor as needed |   |
| Patient should be lateral decubitus, with the CSF shunt reservoir facing up. Feel for the reservoir in the valve. Shave hair if needed. Clean the skin and drape the incision site |    |
| Insert a small 23g-25g butterfly needle into the reservoir, until you hear a pop or see CSF flowing. |  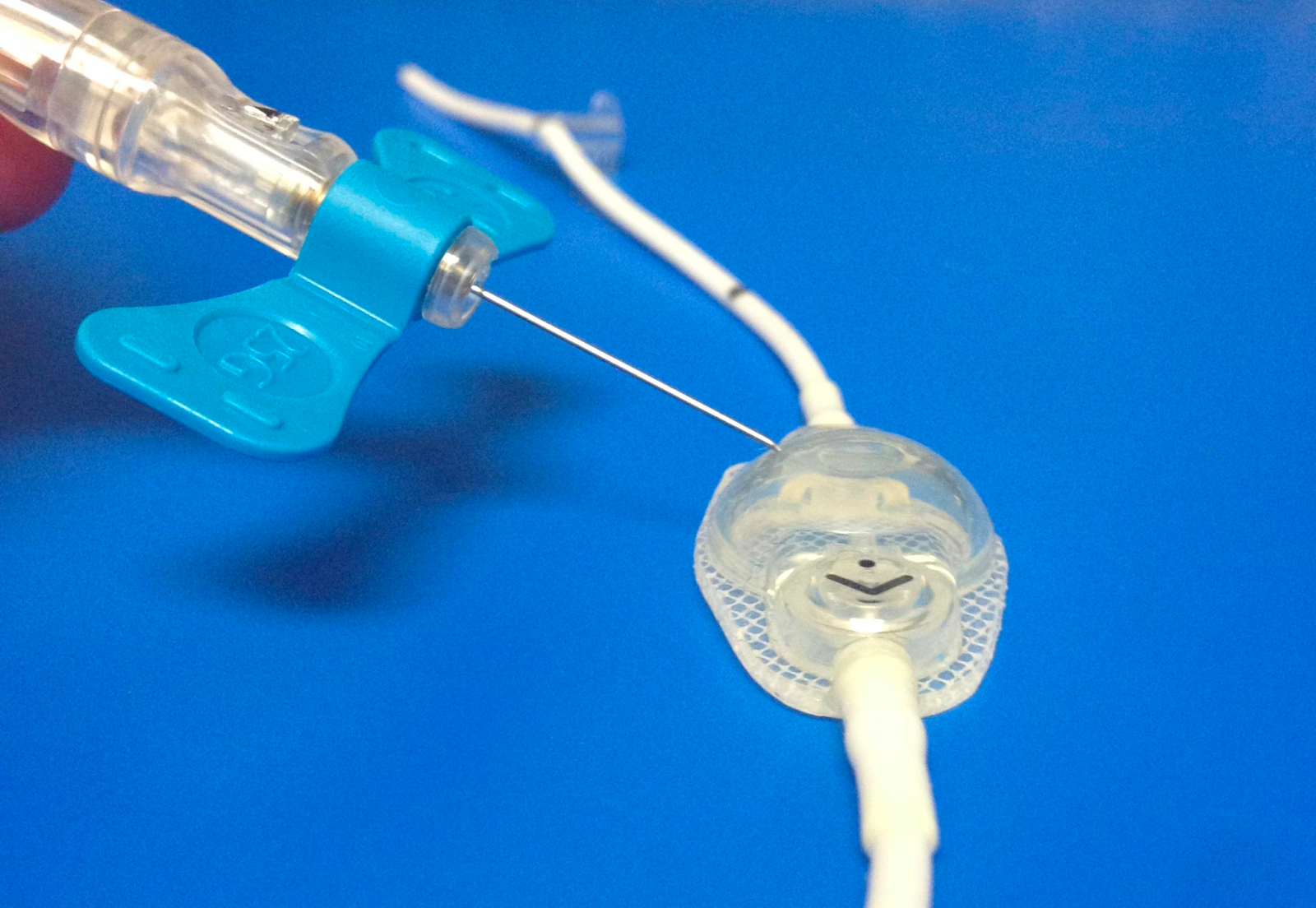  |
| Evaluate for spontaneous passive CSF filling the line of the butterfly needle. If it is not freely flowing, consider aspirating with a syringe. |   |
Measure the opening pressure with a manometer. The manometer should be held at the level of the ear. If ICP>15, attempt to drain until it normalizes. |   |
| Aspirate CSF with syringe. Collect 5 mL of CSF and place into sterile specimen containers |  |
| Withdraw needle, and place gauze to site. Send the cerebrospinal fluid sample for cell count, glucose, protein, gram stain, and culture |
For further reading, check out:
Tintinalli Chapter 14: CNS procedures and devices
http://www.emdocs.net/complications-csf-shunts-ed-presentations-evaluation-management/
https://dontforgetthebubbles.com/vp-shunts/
https://www.ncbi.nlm.nih.gov/books/NBK459351/
