Case Summary:
22 y/o M no pmh p/w painless jaundice x 5 days in the setting of recent febrile illness 1 week prior and taking Tylenol 1g q6h for several days.
Physical exam was positive for jaundice, otherwise normal.
Notable lab findings include:
HepA IgM positive
Elevated LFTs with ALT in 1400s
Coags normal
APAP level negative
VBG/BMP normal
US RUQ normal
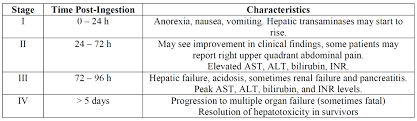
The patient was ultimately determined to be in Stage IV APAP toxicity and happened to have labs from the day before. When the labs were trended, it was adequate to make the determination that the ALT had already peaked. Pt had a score of 0 on the King’s College Criteria for APAP toxicity. This patient was discharged from the ED.
Takeaways:
Jaundice Differential
| Prehepatic Increased bilirubin production | Hepatocellular Impaired hepatocyte function | Cholestatic Obstruction of biliary system |
| Impaired bilirubin conjugation (Gilberts Syndrome) Hemolysis
|
|
|
APAP (Acetaminophen) Toxicity
- 50% are intentional, 50% are unintentional, you should have a low threshold for psych eval
- The rule of 150’s can help remember toxic dosing
- Toxic dose is 150mg/kg
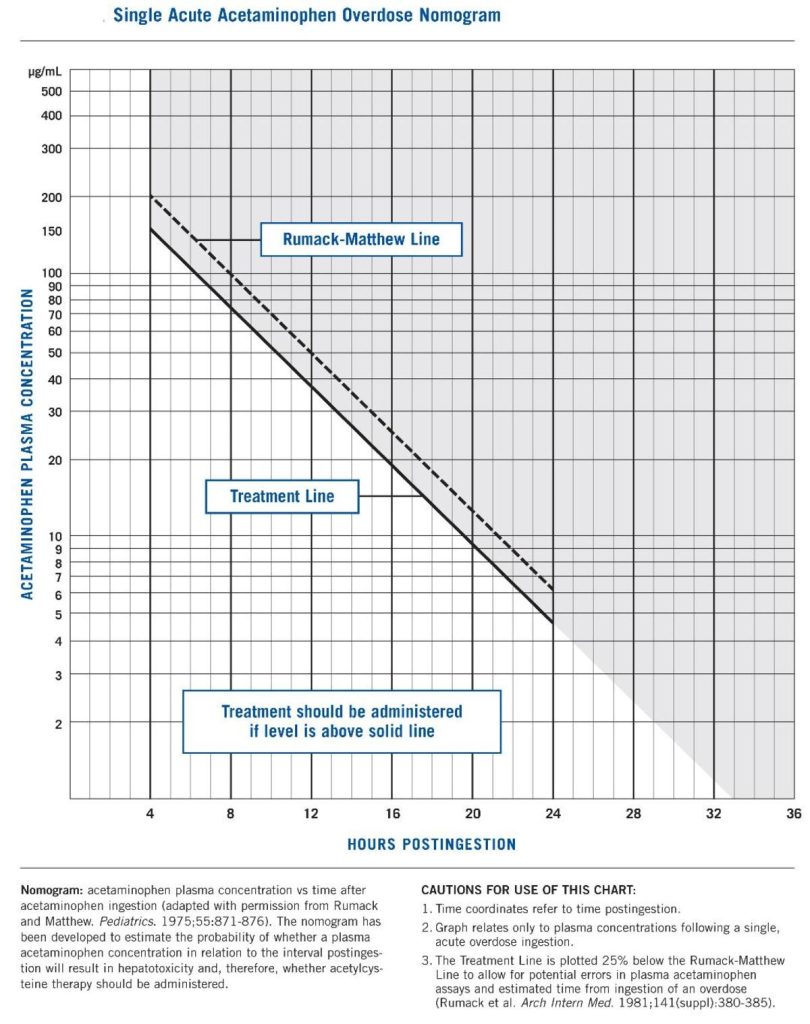
- Give NAC if level is > 150mcg/mL 4 hours after ingestion
- Initial loading dose of NAC is 150mg/kg IV
- There are different stages of APAP toxicity, and can be determined based on time, and symptoms as well as labs
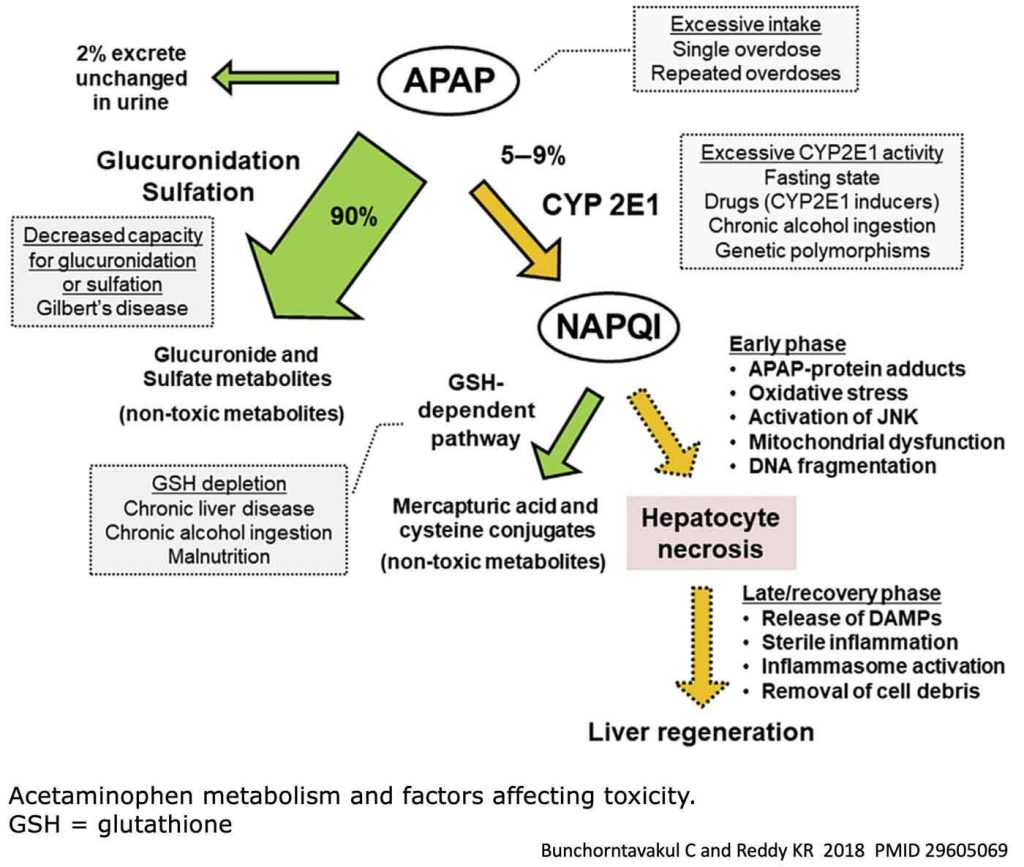
- There are several factors that affect APAP metabolism including but not limited to CYP2E1 inhibitors, fasting states, chronic EtOH ingestion, malnutrition and prior genetic predisposition…in other words, chronically malnourished or EtOH users have a lower threshhold of toxicity
- The King’s College Criteria for Acetaminophen Toxicity can be used to determine the need for referral or transfer for liver transplant. The components of this tool include INR, arterial pH, Creatinine, and hepatic encephalopathy. (LFTs are NOT considered, and neither is APAP level)
- The Rumack-Matthew Nomogram can help you determine whether or not to start NAC, however is only useful iin the first 24 hours, with a suspected acute ingestion. (Stage 1 only).
- N-acetylcysteine (NAC) is the antidote for APAP toxicity.
- It acts as an antioxidant and decreases hepatic necrosis.
- When given correctly within the first 8 hours of ingestion, it has 100% effectiveness.
- It is safe during pregnancy
- About 4-17% of people will have an anaphylactoid reaction (not true anaphylaxis…proceed with treatment!)
- Standard dosing is a 21-hour protocol
- Loading dose 150 mg/kg over 1 hour
- Followed by 50 mg/kg infused over 4 hours,
- Followed by 100 mg/kg infused over 16 hours
