Intro:
- Stroke is the third leading cause of death and number one cause of disability in the United States.
- Classically, strokes present with sudden onset focal neurological deficits in a vascular distribution and need prompt assessment and management to re-establish blood flow and avoid brain damage.
- However, the diagnosis of stroke is not always straightforward.
- Up to 1/3 of strokes diagnosed in the ED are later diagnosed as stroke mimics, which present similarly to strokes, but are not. Up to 15% of stroke mimics are treated with tPA.
- Thus, stroke mimics are important to understand in order to avoid inappropriate and potentially harmful medications and interventions.
What are some classical stroke syndromes?
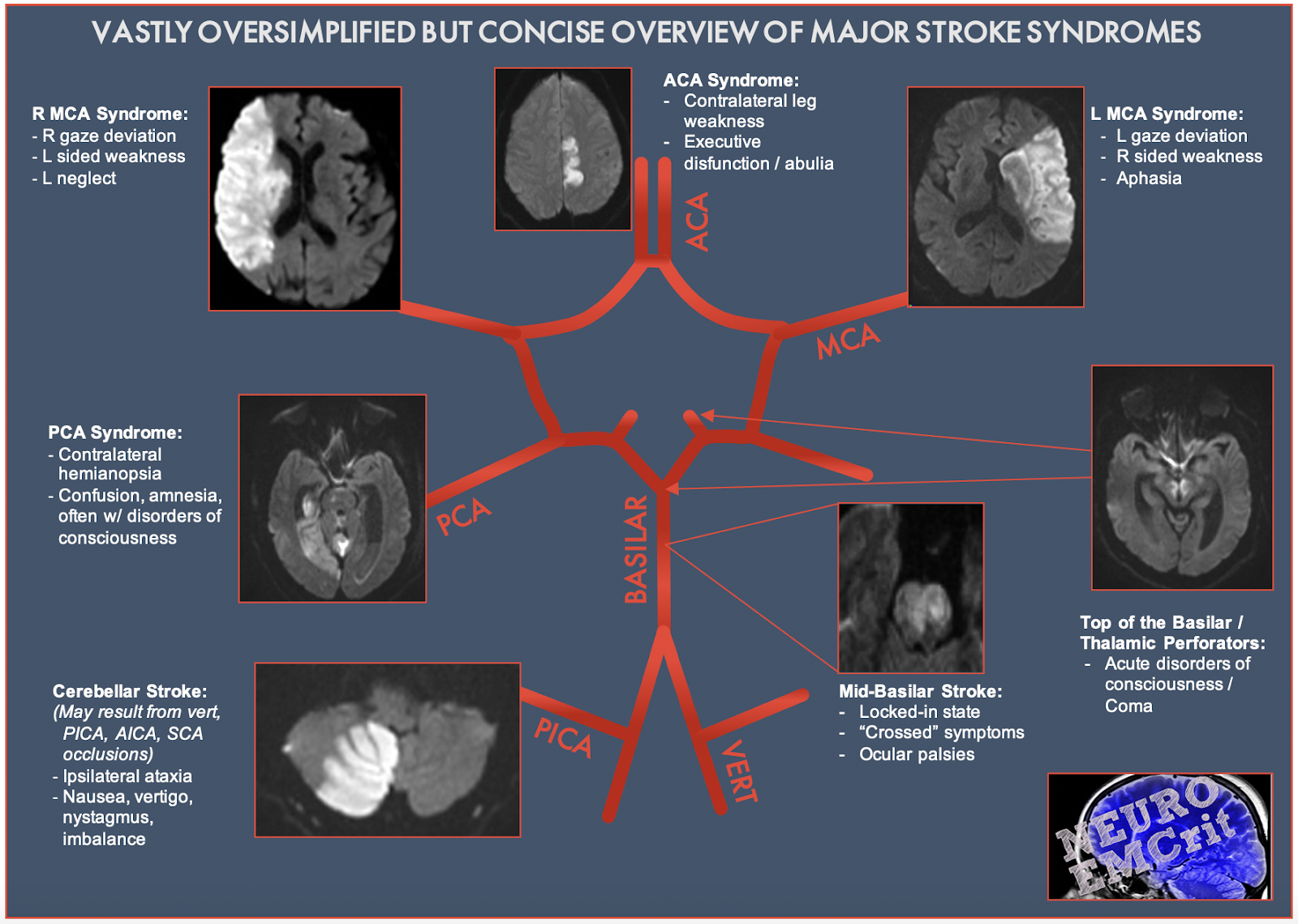
There are many complicated stroke presentations (a whole residency and fellowship dedicated to this), but we will review just four classic, simplified stroke presentations here. Please enjoy my stick figure art, inspired by our colleagues at Ottawa EM, at and these nice graphics with radiology findings from EMcrit.
- ACA
- MCA
- PCA
- Lacunar strokes
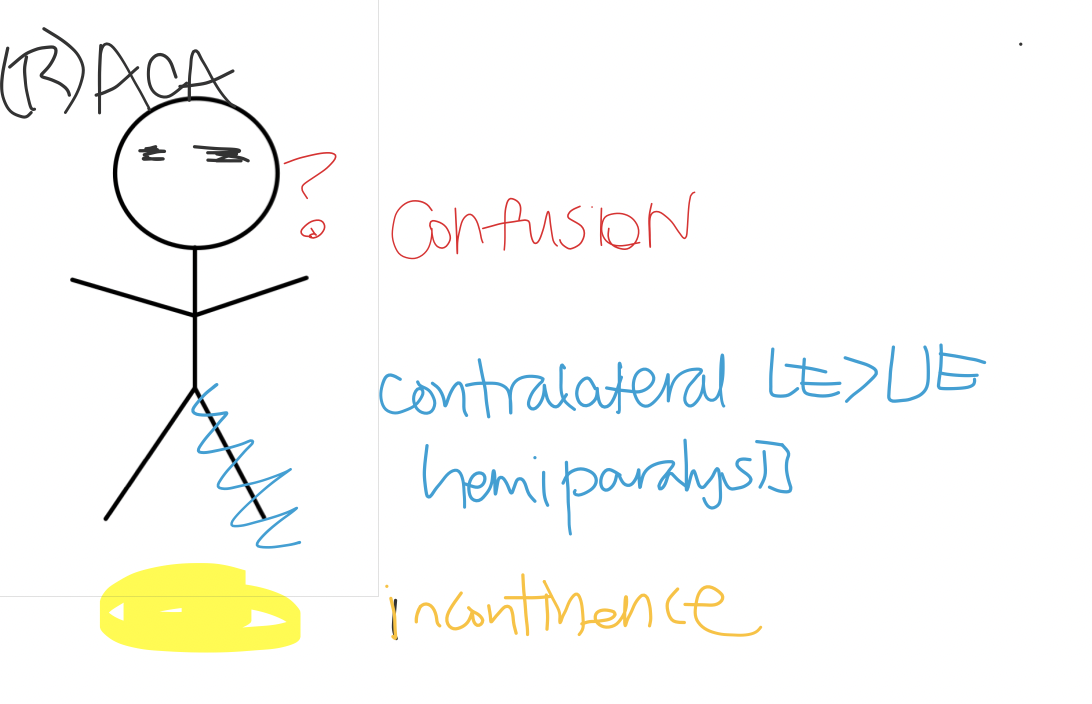 ACA stroke (affects frontal lobe) – AMS/Abulia – Contralateral LE >UE hemiparalysis – Apraxia or clumsy gait – Incontinence | 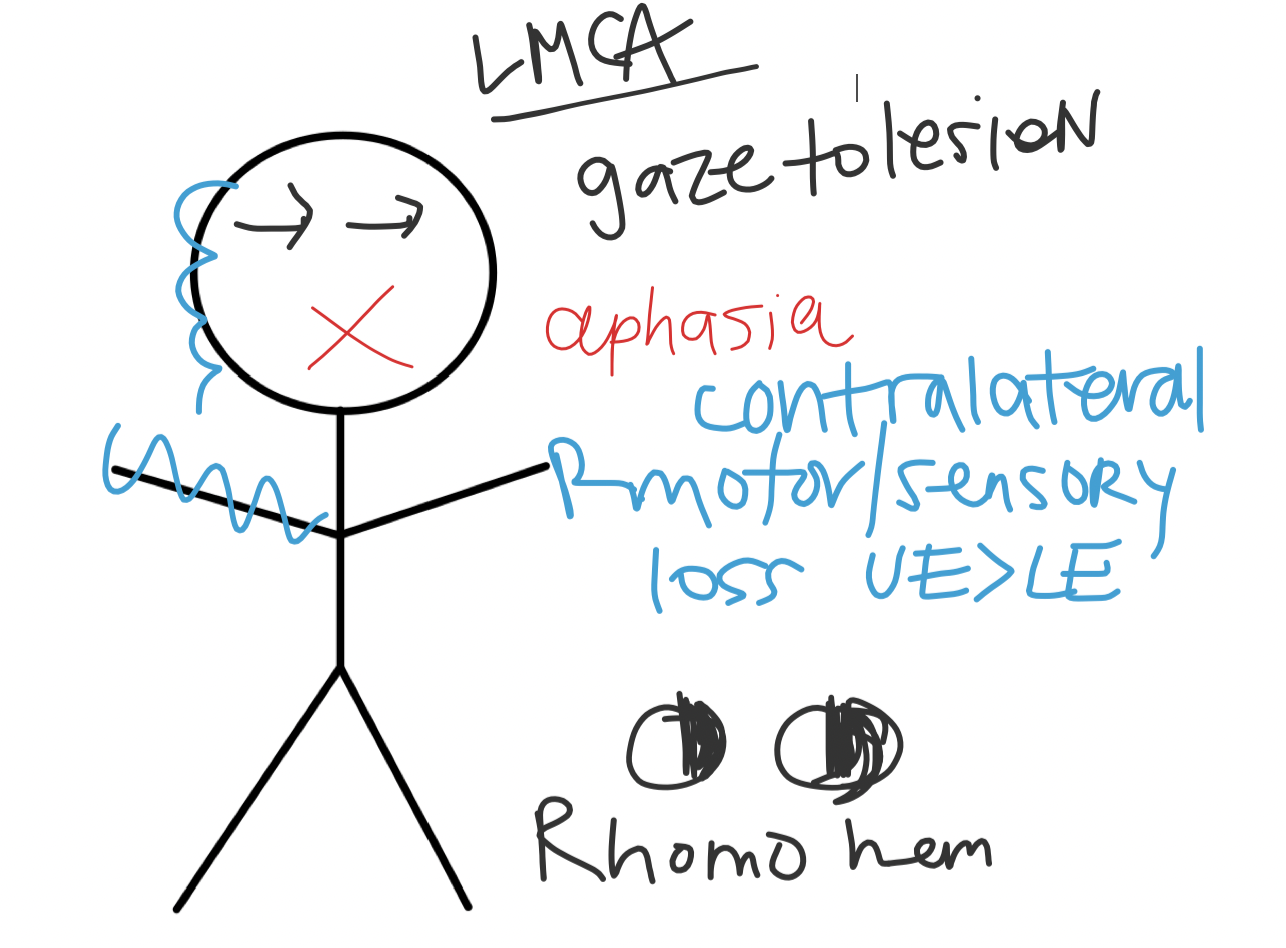  MCA stroke (affects frontal/temporal/parietal lobes) – Contralateral motor and sensory symptoms face & UE>LE – LMCA: expressive or receptive aphasia – RMCA: hemineglect – Gaze preference toward lesion – Homonymous hemianopsia |
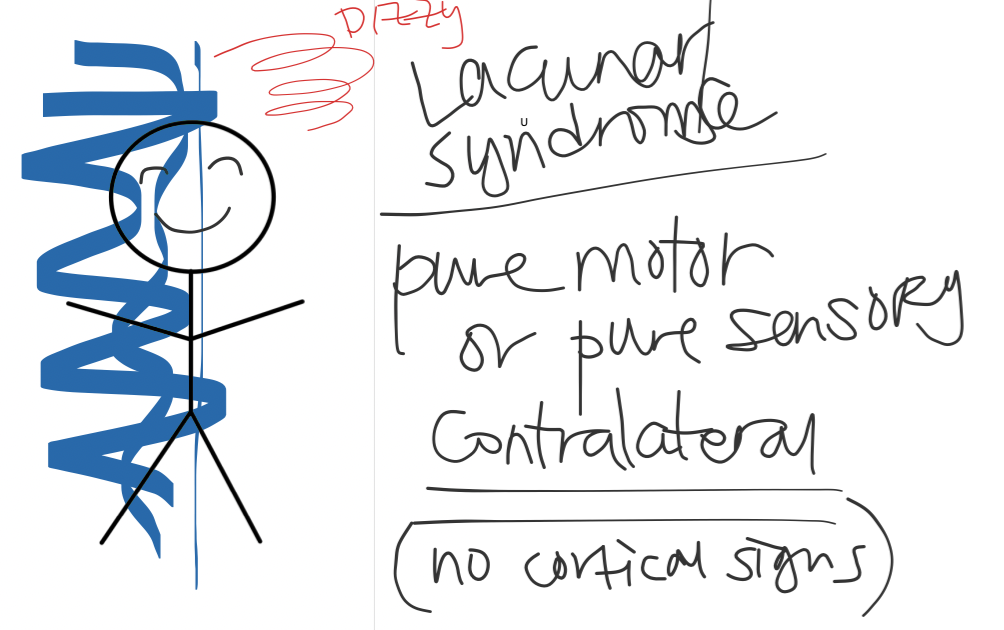 Lacunar stroke – These smaller vessels are deeper within the central nervous system – Contralateral stroke: pure motor, pure sensory, sensorimotor lacunar, ataxic hemiparesis, dysarthria and clumsy-hand syndrome. |  – PCA stroke (Occipital lobe) – Vertigo – AMS – Visual field defects |
What is more likely to be a stroke vs. mimic?
- Looking at the literature – One of the first papers that reviewed variables that can help in the diagnosis of a stroke was done in 1995 by Libman, et. al. They looked at 411 patients and calculated the odds ratios of strokes based on features from history and physical exam.
- Overall, none of the ORs were very high, but they concluded that abnormal eye movements, increased systolic BP, diastolic blood pressure greater than 90 mm Hg, and a history of atrial fibrillation or angina increased the odds of stroke and decreased the odds of a mimic.
- They also suggested that decreased level of consciousness, cognitive dysfunction, and normal eye movements were predictors of mimics, and that patients with stroke mimic were younger, likely female, and were without risk factors (atrial fibrillation, hypertension, and hyperlipidemia).
- Another study was published in the Journal Stroke in 2006, by Hand, et. al found similar results, concluding that loss of consciousness, history of cognitive impairment, seizure at onset, and the absence of lateralizing symptoms were the best predictors of stroke mimics. They also noted that while that eye deviation, while with a large confidence interval, was found to have a significant predictive value for stroke.
- Thus, while the literature does conclusively identify any “pathognomonic” features, it does help physicians think when they should consider stroke mimics on the differential.
That being said…what are common stroke mimics? These can be divided into medical and functional/conversion disorders.
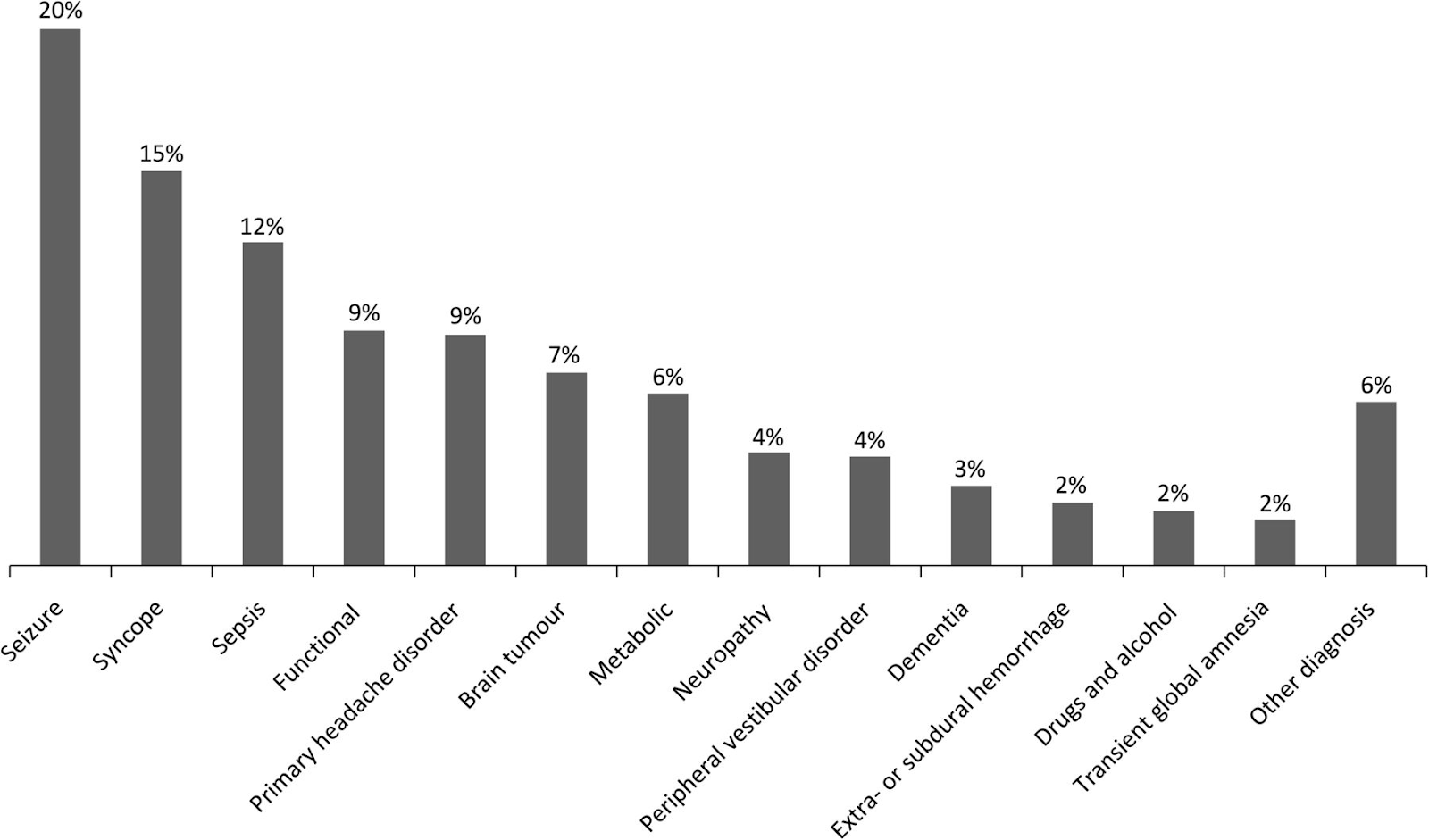
- Medical (in order of most common to least)
- Seizures: Focal seizures are common and may be seen in patients with prior strokes. Todd’s paralysis or post-seizure paralysis can be brief or prolonged, and can happen with any seizures – even alcoholic withdrawal seizures.
- Syncope: This is when patients have abrupt and transient LOC, absence of postural tone, with rapid and complete recovery! This is caused by global interruption of blood flow to the brain. Usually cardiac causes > neurologic. If neurologic etiology for syncope it is usually more seizure>stroke, but consider neurologic stroke if there’s double vision, complete vision loss, and/or vertigo.
- Sepsis: Most common mimic is from urosepsis, and this presents often as confusion or agitation/somnolence. Sepsis, however, does increase your risk for stroke, so look for asymmetric findings, aphasia and acute changes in mental status before attributing the symptoms purely as from sepsis.
- Functional: (see below)
- HA/Complex Migraine: Symptoms are often “positive,” unlike “negative” like in strokes, and can include paranesthesias, and visual phenomenons likeal scotomas. Note, these are gradual in onset with “slow march” through different vascular territories. There can be something called migrainous infarcts, where auras become permanent, but these are extremely rare.
- Tumor/mass lesions: These includes hematomas, abscesses, and tumors and present with slow progressive deficits, progressing over days to months. However, one study demonstrated that 6% of patients with brain tumors presented with symptoms <1d, likely 2/2 to hemorrhage or obstructive hydrocephalus, so always consider stroke still on your differential.
- Metabolic (ex: Hypoglycemia): Global metabolic abnormality can present with asymmetric neurologic findings! Hypoglycemia can exclude patients from tPA, which is another reason why we get a rapid fingerstick for stroke codes.
- Neuropathies
- Bell’s Palsy – most common cause of unilateral facial paralysis, evolves over hours to days in younger patients. These patients can have increased auditory changes, increased lacrimation, upper/lower face, and can’t completely close their eyelids. Note, these are rarely associated with sensory changes.
- Saturday night palsy
- Peripheral vestibular disorder – The presence of brainstem signs (dysarthria, diplopia, ataxia, weakness and numbness) can help differentiate between peripheral or central mechanisms, but are not always present.
- Transient Global Amnesia: Presents with sudden development of anterograde amnesia with no loss of consciousness, seizures, or other focal deficits. Thus, your neurologic exam is normal except for the memory deficit. Unfortunately, the etiology is uncertain. Triggers include severe stress, physical activity, and headaches.
- Other:
- Multiple sclerosis (MS) – Acute MS can occasionally be mistaken for acute stroke. Younger age, prior history and multiple abnormalities on neurological assessment can point you to this diagnosis, but may be especially difficult if it is the first attack of MS. That being said, studies suggest that the risk of stroke is increased by 28% in MS so consider it on your differential.
- Post-stroke recrudescence (PSR) – This refers to the re-emergence of previous stroke-related deficits in the settings of metabolic, infectious and toxic dysfunction. This is rare but does occur. The diagnosis requires an MRI which shows the old stroke.


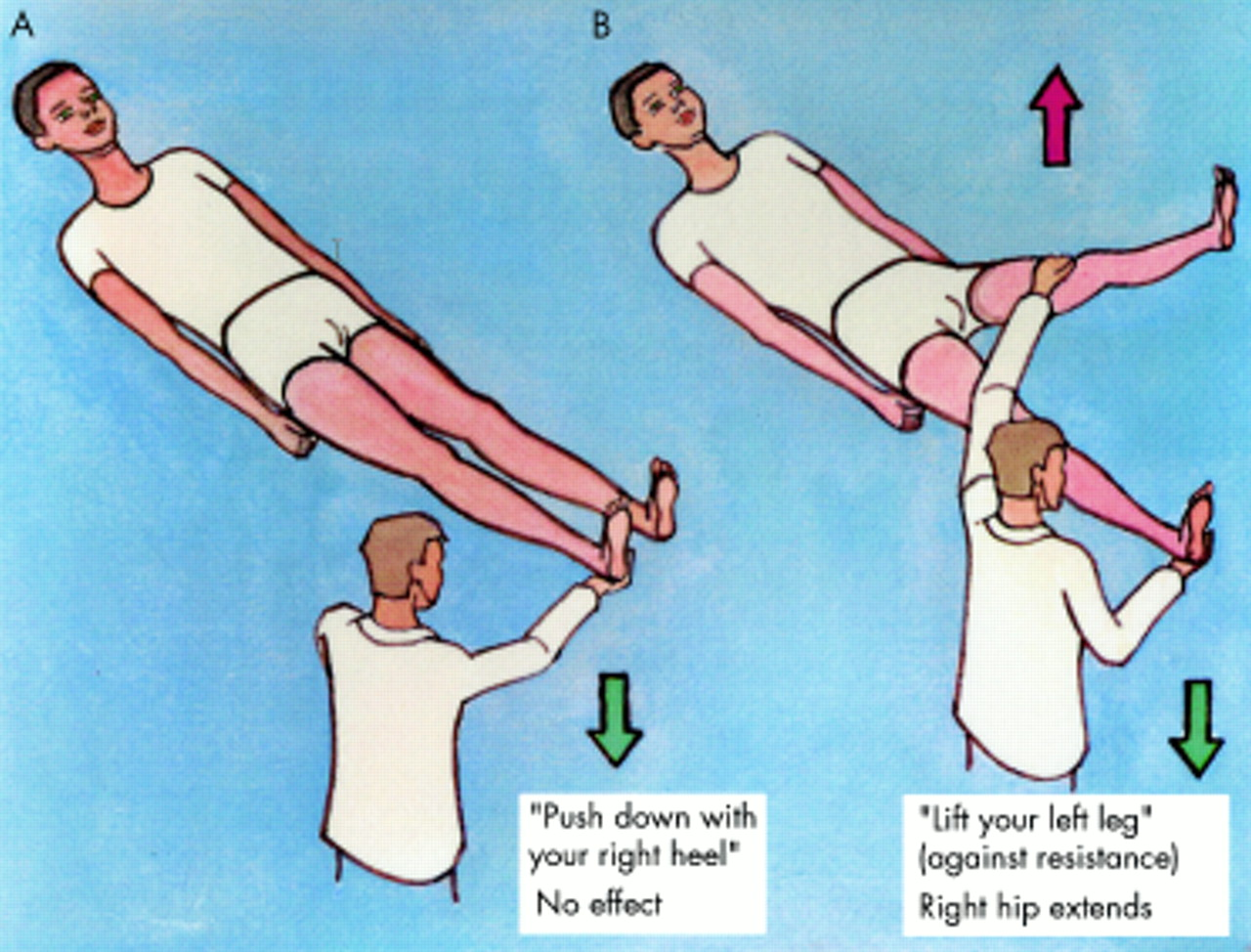
Conversion disorder/Functional – This is different from malingering, as this is not deliberate! You should still call a stroke code if the patient is in the time window for tPA/thrombectomy. However, demonstration of a Hoover’s sign and drift without probation can suggest a functional etiology.
- Downwards drift without pronation
- This has a specificity 100%, sensitivity 96% for functional weakness
- The arm drifts down, but no pronation!
- Counts as pronation if the 4th/5th fingers rotate slightly.

What are some uncommon stroke presentations?
- Movement disorders
- Acute hemiballismus can result from an infarct of the mid brain/subthalamic nucleus.
- Dyskinesia: One review article found that any dyskinesia, hypokinetic or hyperkinetic, can be found with ischemic lesions at motor cortical or subcortical regions but it is rare!
- Isolated confusion: Isolated parietal lobe strokes can cause confusion without motor deficits
- Isolated paresthesias – Tingling of arms/face with associated pain. This is often interpreted as trigeminal neuralgia, or functional or MS, but can be from a stroke in the parietal cortex or in the thalamus. The key is sudden onset with patients with stroke risk factors.
