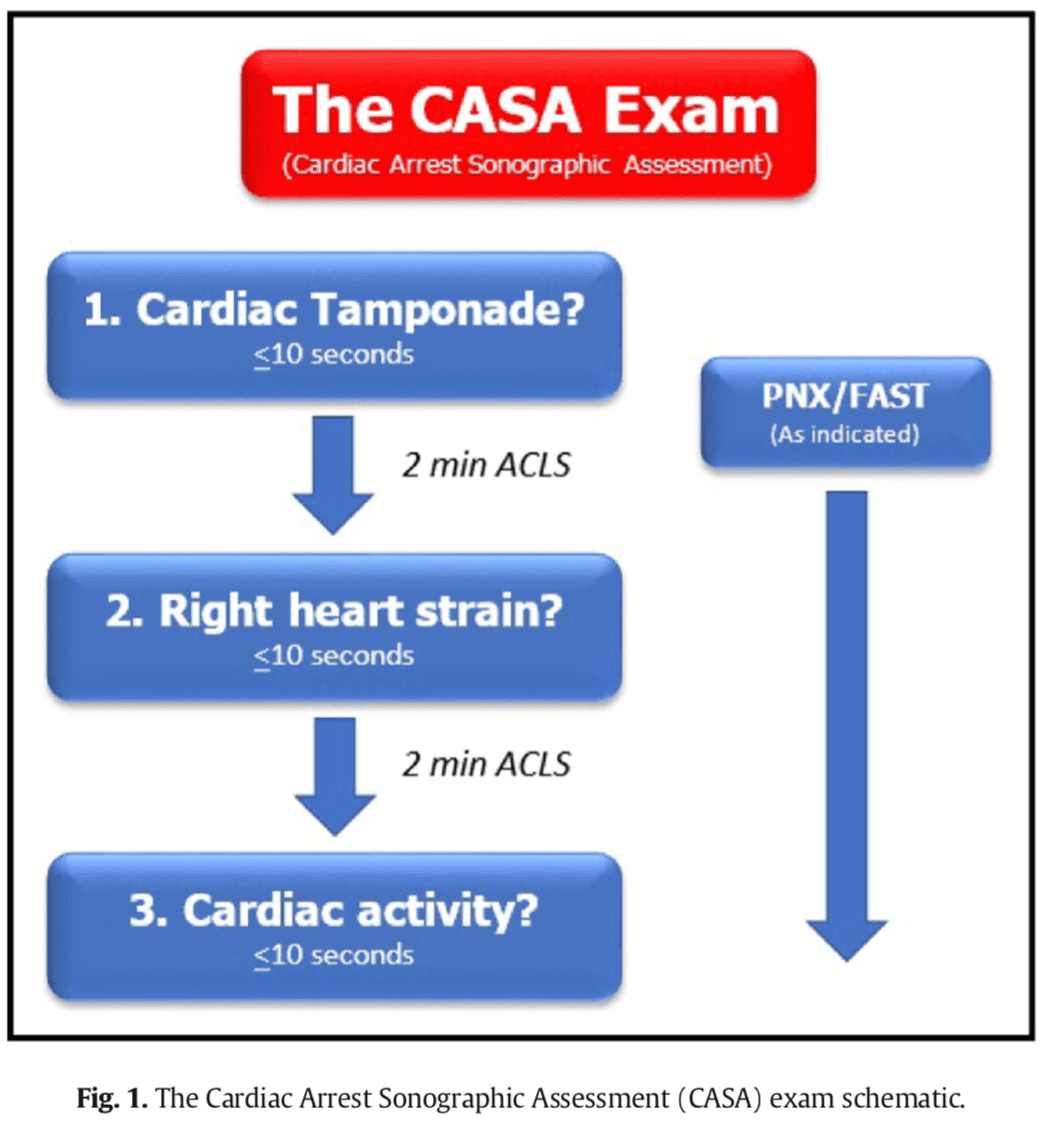
Ultrasound during cardiac arrest has quickly become standard. Initially, data suggested that the use of ultrasound during arrest increased pauses between compressions which worsens outcomes. To decrease time between compressions, many protocols were proposed (see here). One such protocol that successfully decreased time between compressions is the CASA (Cardiac Arrest Sonographic Assessment) protocol.
The CASA protocol assesses for cardiac tamponade, right heart strain, and cardiac activity. It emphasizes one view per pause between compressions with either the subxiphoid or parasternal long view. (The subxiphoid view seems to be the default primary view to look for). The ideal view depends on the patient’s comorbid conditions such as COPD, obesity, cachexia, etc.
Rapidly intervened-upon cardiac tamponade in PEA during cardiac arrest has significantly higher hospital discharge rates. Evidence of right heart strain is important but the evidence of fibrinolysis during arrest is mixed with many studies showing no 30-day mortality benefit to lysing during a code. Finally, patients with PEA and cardiac standstill on ultrasound have a 0.0%-0.6% survival to hospital discharge rate.
Bottom line: Ultrasound in cardiac arrest is useful, you should have a protocolized method for using it to minimize pauses between compressions and maximize the information you obtain, & combining this with other data such as downtime, CPR in the field, & initial rhythm will help prognosticate and guide management.
Some microskills for this POCUS:
- As team leader, assign someone to do the POCUS
- Place the ultrasound probe on the chest during compressions to identify your optimal window for when compressions are paused – this has been shown to decrease CPR pause length
- Keep a towel or a chuck nearby to wipe down the patient and the probe in between the POCUS as the area can become slippery quickly
There are many benefits to using ultrasound during a code. Ultrasound can also help identify hypovolemia, pneumothorax, pleural effusions that could be worsening hypoxia, and much more. For example, here, Scott Weingart says that “PEA is stupid” & also talks about PEA vs Pseudo PEA with the difference noted on ultrasound. Look here for a deep dive on PRES vs PREM (Pulseless with a Rhythm and Echocardiographic Standstill vs Pulseless with a Rhythm and Echocardiographic Motion).
Ultimately, given the heterogeneity of studies in terms of timing & application and definition of cardiac motion, ultrasound is considered an adjunct to CPR with a class 2b recommendation in the 2020 AHA guidelines. I think it is likely that ultrasound will have a codified roll in cardiac arrest in future AHA guidelines & being proficient with a standardized ultrasound exam is a beneficial source of information during cardiac arrest.
Yours in ultrasounding,
Shivam