Tuberculosis in the ED
Patient presents to Elmhurst ED with cough, hemoptysis, night sweats and fatigue – quick, what’s the first diagnosis that comes to mind?
This is the classic presentation for tuberculosis. But several times now I have been surprised by less typical symptoms of TB. So I thought it might be helpful to review how TB might present in the ED, especially since some estimates say that ⅓ of the world’s population is infected. And the populations at highest risk – residents from endemic regions (especially India, China, the Philippines, Pakistan, Nigeria, Bangladesh), unhoused persons, those in institutional living or employment (prisons, shelters, nursing homes, hospitals), the elderly or very young, and immunosuppressed – are people we see very often in our EDs.
TB is caused by the acid-fast bacillus Mycobacterium Tuberculosis and spreads via aerosolized respiratory secretions. It migrates into the lung alveoli, activating the host’s defense mechanisms. So its presentation often depends on the host’s immune system.
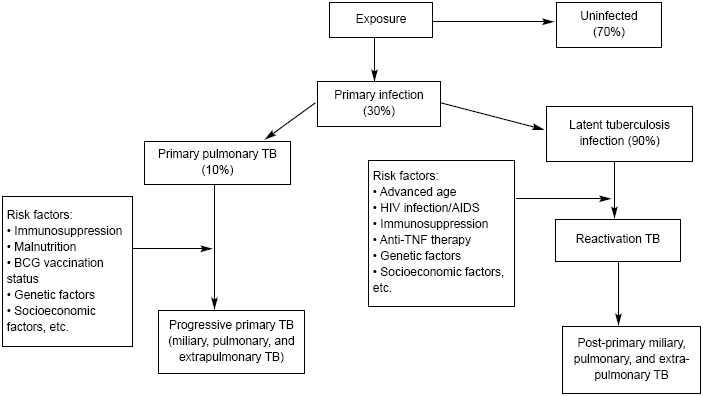
Adapted from: Sharma SK, Mohan A, Sharma A, et al. Miliary tuberculosis: New insights into an old disease. Lancet Infect Dis 2005;5:415-430.
Let’s start from exposure. Out of those with primary infection, most patients’ immune systems can contain the organism in regional lymph nodes, leading to latent TB. Primary pulmonary TB is usually asymptomatic. Only 10% of patients with primary infection will present with pulmonary TB symptoms. In immunocompromised patients, these primary symptoms can be rapidly progressive.
Similarly, patients with latent TB who are at high risk may experience reactivation of previously contained focus.
Here’s a list on how TB might present:
| Region | Symptoms | Imaging | |
| Pulmonary – apical and posterior upper lobes, superior segment of lower lobe | Productive cough, dyspnea, hemoptysis, pleuritic chest pain Immunocompromised may have more atypical findings |  | |
| Lymph | Tends to be unilateral and non-tender Can develop scrofula= enlarged cervical nodes that sometimes rupture and form fistulas |  | |
| Pleural | Pleuritic chest pain, cough, and unilateral pleural effusion on CXR | 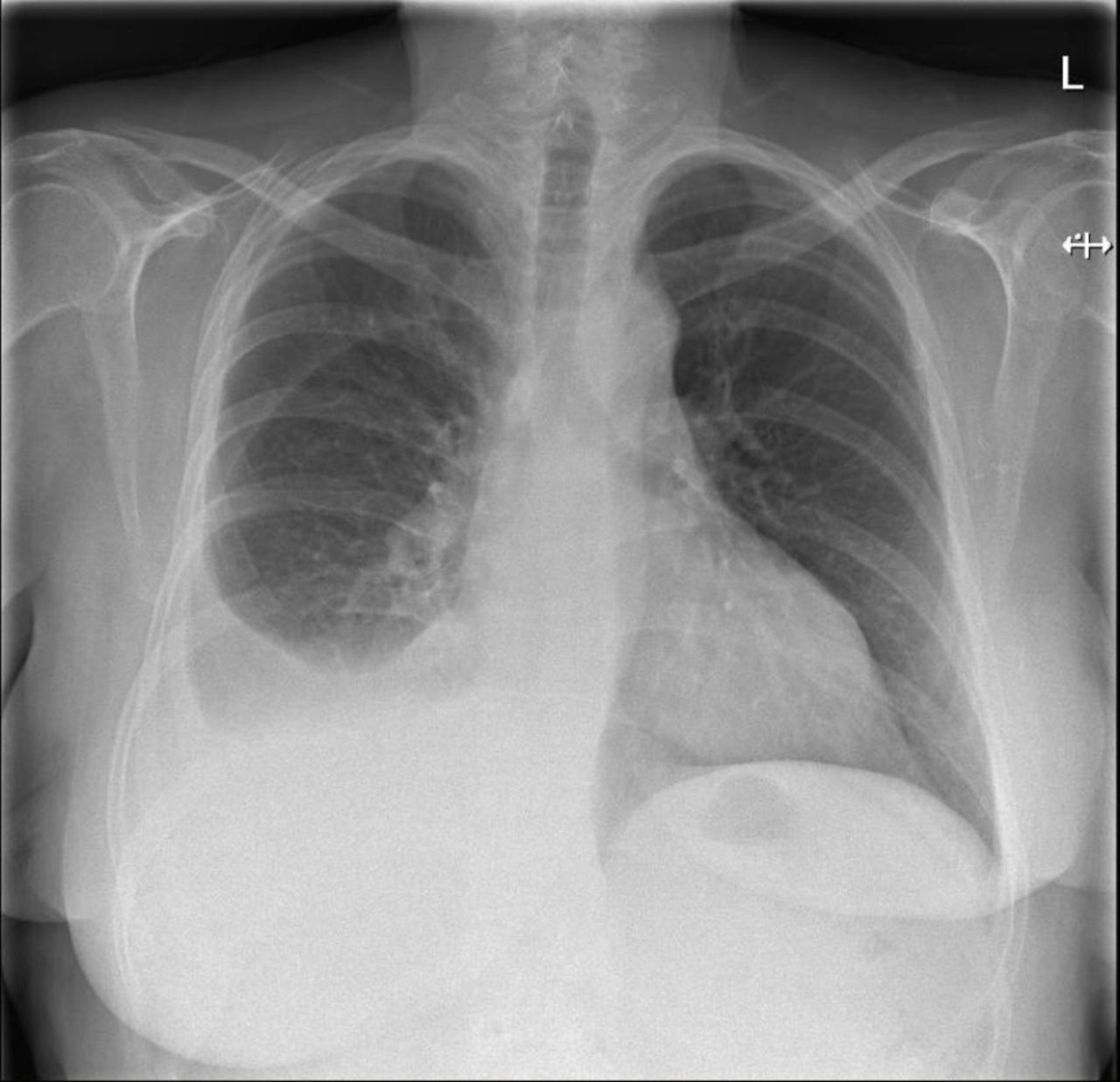 | |
| CNS | 1: Indolent h/a, fever, AMS2: meningitic phase3: paralytic phase | 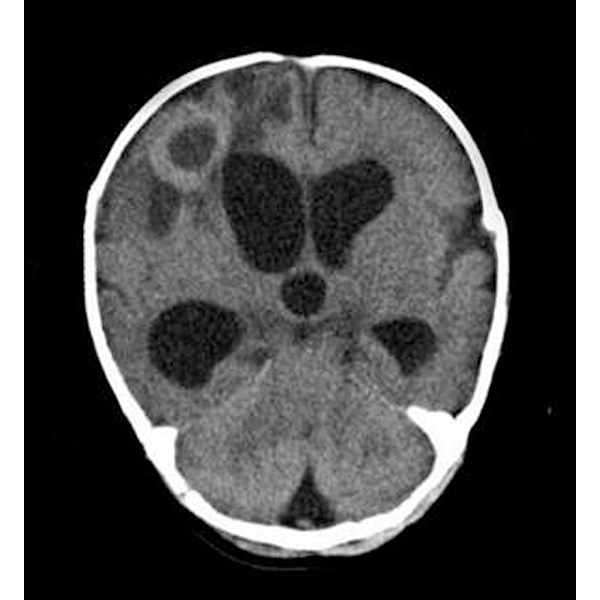 | |
| Peritoneal | Ascites, abd pain, weight loss, fever | 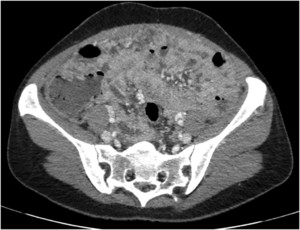 | |
| Pericarditis | Constrictive |  | |
| Adrenal | Usually bilateral, may present in shock Consider steroids! |  | |
| Skeletal | Most commonly thoracolumbar spine, osteomyelitis (Pott’s) |  | |
| Miliary (Disseminated) | Wide hematogenous spread, often with multi-organ failure and shock |  |
Next steps when you suspect TB:
- Isolate in negative pressure room
- Get CXR and quant-gold (culture is definite but won’t come back in ED)
- Report to public health services
- Consent for HIV co-testing
- Baseline labs for treatment: CBC (platelet), LFTs, serum urea, creatinine
- Don’t initiate treatment unless in consult with ID
Discharge instructions: home isolation procedures and follow up at appropriate clinic
Admit: uncertain dx, noncompliant, concert for multidrug resistant, or severe illness with respiratory compromise, shock, or multi-organ failure
www.emdocs.net/tuberculosis-presentation-ed-management/
https://emedicine.medscape.com/article/358610-overview
https://www.jpeds.com/article/S0022-3476%2817%2930889-2/pdf
https://casereports.bmj.com/content/2018/bcr-2018-224992
https://www.ajtmh.org/view/journals/tpmd/104/1/article-p223.xml
https://radiopaedia.org/articles/tuberculous-pericarditis
