Intro
Raise your hand if you ever struggled obtaining a CSF sample from a Lumbar Puncture. I “virtually” see that most if not all of you at one point in your career struggled with this.
This pearl is inspired by an overnight Elmhurst A-side shift I had several months ago with a patient requiring a Lumbar Puncture. I waved off my senior/attending and told them “No worries, I got this.” After multiple attempts, I made the walk of shame back to my team telling them I couldn’t obtain a sample.
As Emergency medicine doctors, we rely on ultrasound for so many procedures (central venous access, pericardiocentesis, paracentesis, etc..), so why not for Lumbar Puncture. In this TR pearl, I will teach you some skills/pearls you can take to your next difficult LP to make this often difficult “blind” procedure into one that is easier and precise.
Tl;Dr < 5 minutes
Ultrasound guided LP increases the rate of success while decreasing procedure time, passes with needle, and pain score
Use Ultrasound to only identify anatomy. It should not be used in real-time. You will use the transverse and longitudinal plane to identify the
- Midline
- Spinous Process
- Ligamentum Flavum
Extended Pearl > 5 minutes
What is the purpose of using a POCUS guided Lumbar Puncture?
In a meta-analysis of almost ~1,000 patients comparing a “blind” approach vs a POCUS guided approach, there was a statistically significant increase in success rate as well as decrease in procedure time, fewer passes with the needle, and decrease in pain score.
Consider using this technique in patients you anticipate being a difficult LP (i.e cannot palpate the spinous process). Examples include patients who are obese, have history of OA/DJD, ankylosing spondylitis, previous back surgery, and kyphoscoliosis.
What is the anatomy I am thinking of when I am performing an LP? What is the position of the patient?
You can have the patient either in the 1.) Seated 2.) Lateral decubitus position with the hips flexed towards the abdomen to help open up the intervertebral space. You want to first identify (or the best you can do) the intersection of the “Posterior Superior Iliac Crest” and the midline of the back around the “L3/L4 or L4/5 spinous process.” When inserting a needle, you will pass through the 6 structures as described in the diagram below until you obtain a CSF sample.

What probe/settings am I using on the Ultrasound?
Ideally you want to use the Curvilinear probe or the Phased Array probe to obtain decent depth and resolution. You want to set the depth to at least 8 cm.
Okay, but how am I actually using ultrasound to help me with the Lumbar Puncture?
You will not be using the ultrasound in real-time but only to identify the anatomy and mark the skin. Think of using the ultrasound similarly as you would for a paracentesis to help you identify the landmarks. It’s as easy as 1, 2, 3…
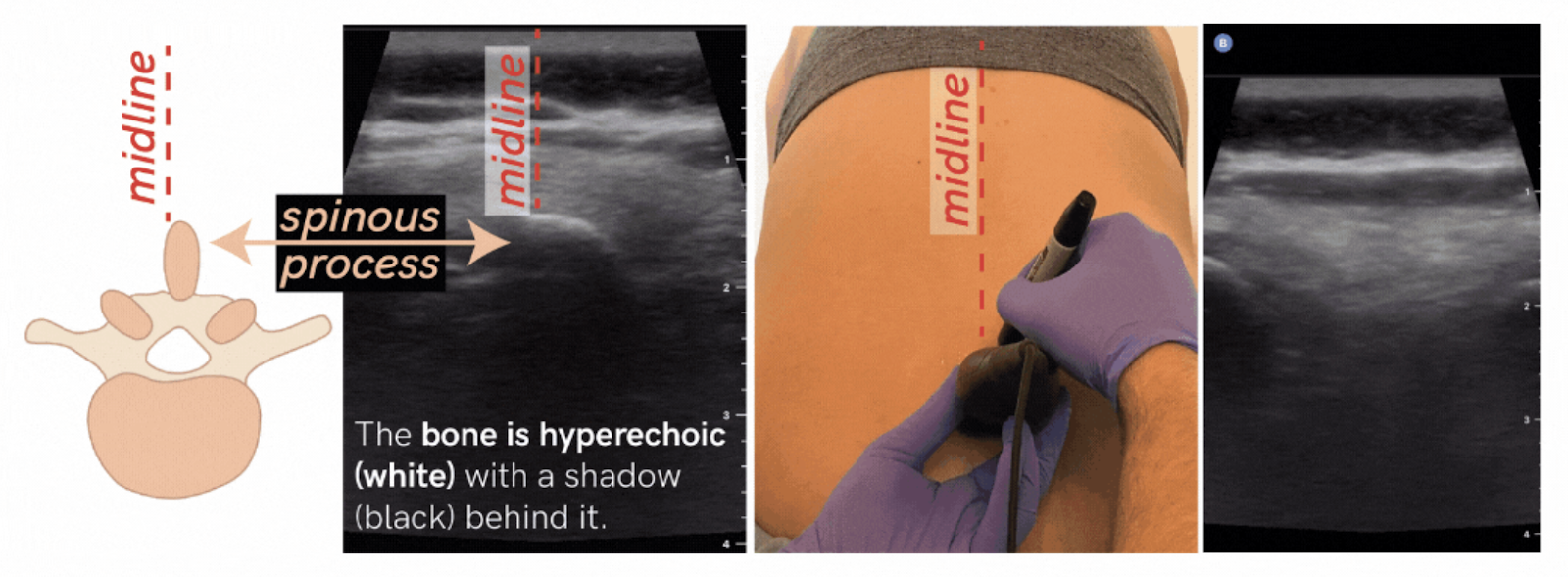
Step 1: Place the probe (curvilinear/phased array) probe in the transverse position to help identify the midline spinous process. The spinous process will be a white hyperechoic structure with shadowing behind it. Do this for several spinous processes to help identify the true midline of the spine.
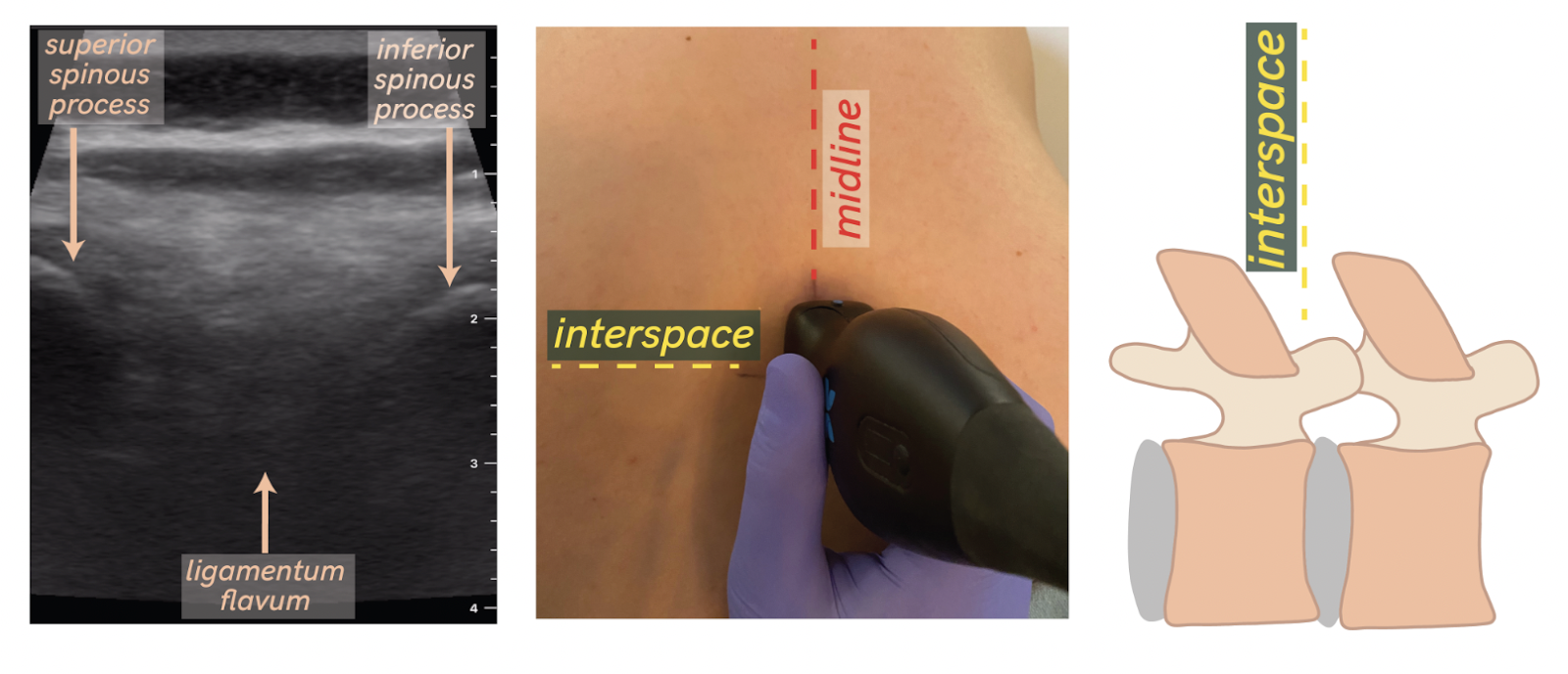
Step 2: Rotate the probe now into the longitudinal plane. You will now see the ligamentum flavum (which is where the target is for the needle) sandwiched by the superior and inferior spinous process (evidenced by white hyperechoic regions). Mark this space which should be perpendicular to the midline line you drew previously. This is the spot where you want to puncture with the needle.
Step 3: Perform the LP as you would normally with the needle directed towards the umbilicus. Rejoice with your team now that you performed a “champagne tap” and successfully did an LP.
Resources
I am attaching resources from which the above diagrams pictures were taken from. In addition, I am including other resources and videos how to further guide you on how to do a normal LP vs POCUS guided LP
