Intro
For this week’s teaching pearl, I wanted to go back and cover a medical pearl. We always hear the word “ECMO” thrown around but I want to today go into a very brief overview of what ECMO is and why it is being used more commonly. I am going to provide the pearl in a Q/A format to make it easier to process.
Disclaimer: This is only a very brief overview of ECMO just so everyone at least has a basic understanding of what the technology is and what the circuit looks like. There are many nuances to the types of ECMO, the placement of the catheters, anticoagulation while on ECMO, ventilator settings, complications, troubleshooting settings etc.. which I will not discuss in this TR pearl but I am more than happy to discuss personally or send you resources. I included several resources including a link to “One pager ICU” which is where my drawing is derived from as well as several podcasts recommended by Dr. Pesyna.
Tl;Dr Brief <5 minutes
Types of ECMO: The two fundamental types of ECMO are Venovenous (VV) and Venoarterial (VA)
Components of the ECMO circuit: Drainage and Return Cannulae, Centrifugal Pump, Oxygenator “Membrane Lung,” Thermoregulator, Sweep Gas Flow/FdO2
Settings you can adjust on ECMO:
To change ventilation/PCO2 – adjust the Sweep Gas Flow
To change oxygenation/PAO2 – adjust the Pump RPM/Blood Flow Rate or FdO2
Extended Pearl > 5 minutes
So what is ECMO?
Extracorporeal (outside of the body) Membrane Oxygenation (device allowing for gas exchange) or ECMO is a technology that provides support by performing the function of a lung and/or heart until those organs can heal or until you can bridge a patient to more definitive therapy.
What are the different types of ECMO?
For the sake of simplification, there are two main types of ECMO.
- Venovenous (VV) = Artificially oxygenated Venous blood is returned to the Venous side (right atrium, after being pulled out from the femoral/internal jugular vein, providing only respiratory support without any circulatory support
- Venoarterial (VA) = Artificially oxygenated Venous blood is returned to the Arterial side, after being pulled out from the femoral/internal jugular vein, providing combined circulatory and respiratory support
What are the Indications and Contraindications for activating the ECMO team in the ED?
Indications: Generally speaking, ECMO is targeted towards the relatively younger and healthier patients who experienced an acute but reversible event that led to cardiopulmonary collapse. Examples include:
- Witnessed cardiac arrest with minimal downtime
- Persistent hypotension or hypoxemia despite maximal conventional therapy/ventilatory management 2/2 to conditions such as PE, MI causing V-Tach/V-fib or cardiogenic shock, drug overdose, etc.
- Severe asthma or ARDS
Contraindications: Generally, ECMO is not targeted for patients with multiple chronic conditions or with multi-organ failure
- Prolonged cardiac arrest
- No identified reversible cause (as you remember ECMO is only a bridge to definitive treatment)
- DNR/DNI
What does the ECMO circuit look like/what are the different parts of ECMO?
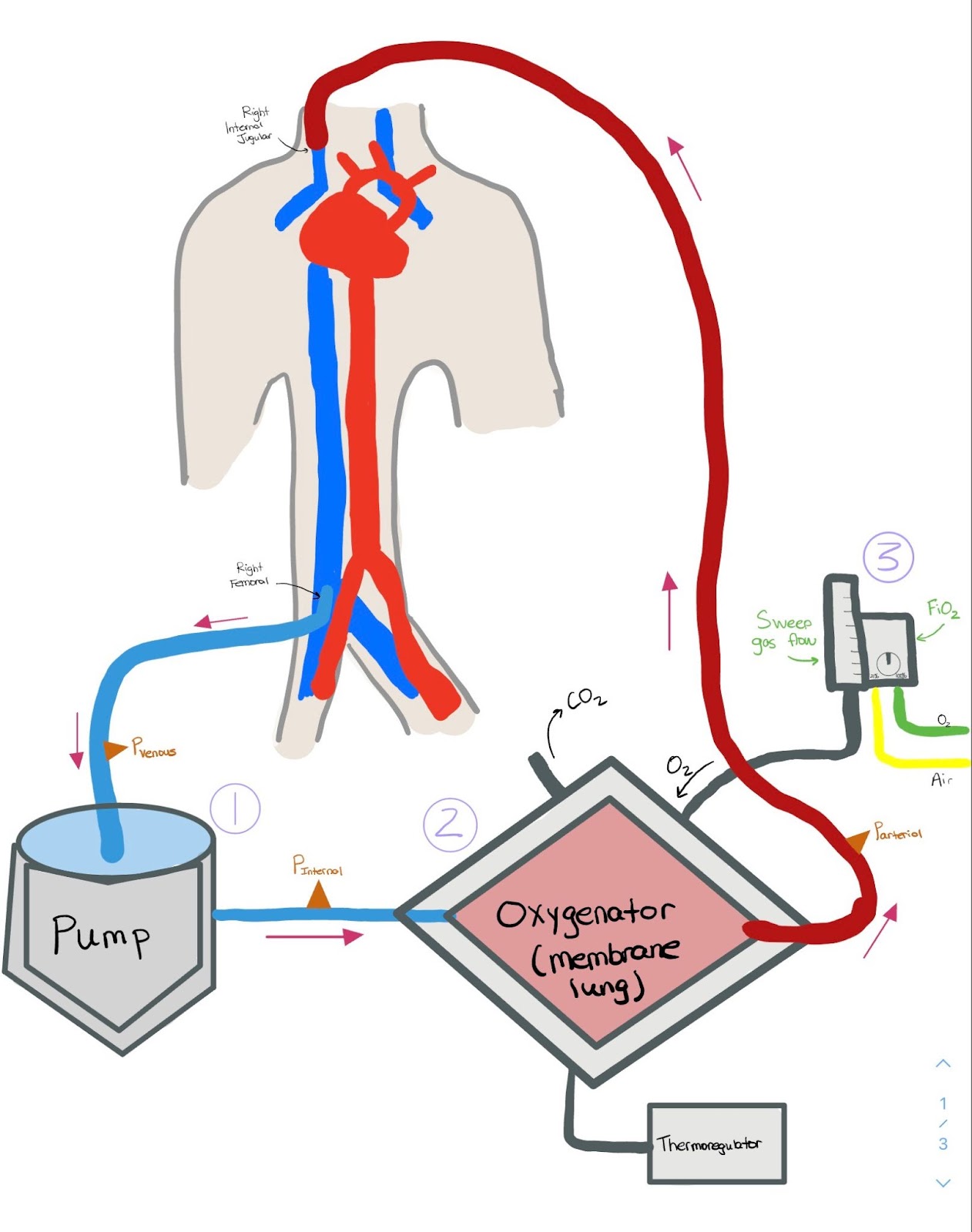
Let’s go through a VV-ECMO circuit with a diagram (I drew it on an iPad so ignore the quality of the drawing derived from ICU-One Pager)
- In this circuit, blood is being drained from the Right Femoral Vein. The Centrifugal Pump is a mechanism allowing blood to be actively pulled. The Pump RPM “revolutions per minute” is a major factor in determining the Blood Flow Rate.
- Blood then enters into the Oxygenator “Membrane Lung.” In this step, gas exchange occurs, where O2 is added and CO2 is removed. The FdO2 which determines oxygenation and the Sweep Gas Flow which determines CO2 removal can both be adjusted here.
- The Thermoregulator/Heat Exchanger helps maintain the blood at an exact specific temperature.
- Blood is then returned to the Right Internal Jugular Vein.
What settings can I adjust in the ED? How can I adjust the ventilation/oxygenation of the circuit?
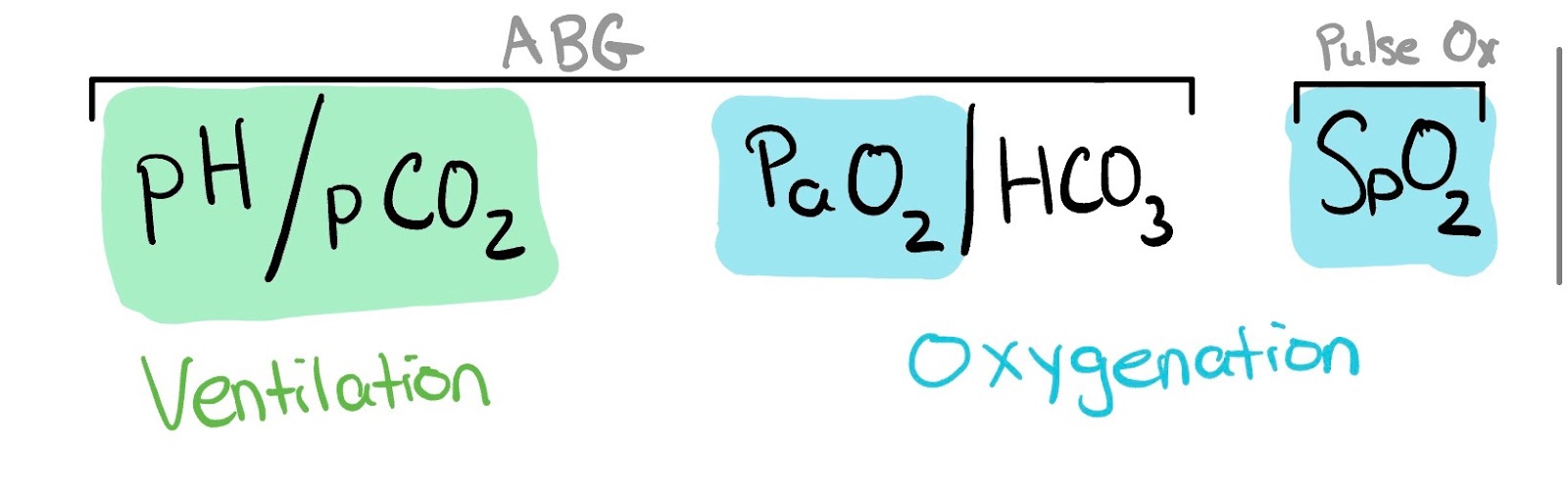
To adjust the ventilation of the system/decrease the PCO2/increase the pH you can increase the amount of Sweep Gas Flow and adjust how much CO2 you want removed from the circuit
To adjust the oxygenation/increase the PAO2 you can increase the Pump RPM/Blood Flow Rate or increase the FdO2.
Where should I place my Arterial line and pulse ox?
In a peripherally cannulated VA ECMO circuit, a right radial arterial line and pulse-ox on the right hand should be placed. Recovery of myocardial function in the setting of poor lung function results in the inappropriate circulation of poorly oxygenated blood and well-oxygenated blood from the ECMO circuit resulting in discrepancy between the upper/lower extremities. Therefore placement of the right radial arterial line and pulse-ox allows for detection of both coronary and cerebral hypoxemia.
How can I activate ECMO at Mount Sinai vs Elmhurst?
Mount Sinai
VA ECMO: 1.) Contact Dr. Greg Serrao (917) – 756 – 6852 or 1-833-MH-SHOCK (1-833-647-4625) 2.) Call the CCU Interventional Cardiology Fellow 3.) Call Dr. Pesyna, Dr. Leibner, Dr. DeVivo, Dr. Andreae if none of the above options are working
VV ECMO: 1.) On Amion call VV ECMO Consult (201-396-9706) under the Institute for Critical Care Medicine – MSH
Elmhurst: Call (212) – 241 – 6467 or 800-TO-SINAI (800-867-4624) to get in touch with the Sinai transfer center to be connected with the ECMO team.
Resources
http://www.emdocs.net/extracorporeal-membrane-oxygenation-ecmo-in-the-ed/
http://accrac.com/episode-33-ecmo-with-dr-rosanne-sheinberg/
http://accrac.com/episode-205-ecmo-update-with-drs-essandoh-cody-and-graul/
